
Social Factors Influencing 1st Line Anti-Retroviral Treatment (ART) Adherence and National Development among Opportunistic Infectious Clinic (OIC) Patients in Harare.
- Mercy Mukumba
- Dr. N. Mutanana
- Dr. U. Goshomi
- 1119-1142
- Mar 22, 2025
- Health
Social Factors Influencing 1st Line Anti-Retroviral Treatment (ART) Adherence and National Development among Opportunistic Infectious Clinic (OIC) Patients in Harare.
Mercy Mukumba, Dr. N. Mutanana, Dr. U. Goshomi
10 Fallon Avenue, P.O.Amby, Greendale, Harare, Zimbabwe
549 Arcturus Road Manresa Harare. Zimbabwe, Box Address: P.O. Box GD 32 Greendale
DOI: https://doi.org/10.51244/IJRSI.2025.12020090
Received: 07 February 2025; Accepted: 18 February 2025; Published: 22 March 2025
ABSTRACT
This study examines social factors affecting adherence to first-line Antiretroviral Therapy (ART) and national development among patients in Harare’s Opportunistic Infectious Clinic (OIC). Using a mixed-methods approach, which combines surveys and interviews, the study identifies stigma, lack of social support, and disclosure concerns as major barriers to adherence. Interventions like peer support groups and stigma reduction programs effectively improve adherence. Since ART adherence improves public health, enhances workforce productivity, and reduces healthcare costs, it plays a crucial role in national development by strengthening economic stability and social well-being. Interventions such as peer support groups and stigma reduction programs have been found effective in improving adherence. Recommendations included targeted interventions, peer support networks, and enhanced family communication to bolster adherence rates among OIC patients. Policymakers and healthcare providers should implement stigma reduction campaigns, integrate psychosocial support into routine HIV care, and strengthen partnerships between healthcare facilities and community organizations to improve adherence and treatment outcomes.
Key Words: ART adherence, HIV/AIDS, Opportunistic Infectious Clinic (OIC), Social determinants, Stigma, Social support networks
INTRODUCTION AND BACKGROUND
ART requires patient compliance not only for the benefit of the patient but also for the societal and economic well-being of the country. Concerning HIV/AIDS, it is vital to sustain the highest percentage of adherence to be able to control the virus and prevent the further spread of the disease (World Health Organization, 2016). ART adherence supports economic growth through its positive impact on health which enables employees to stay productive and healthy while missing fewer days of work and decreasing healthcare expenses. ART adherence promotes social inclusion through its reduction of HIV stigma which allows individuals to access education gain employment and engage in their communities. When people in resource-limited contexts such as Zimbabwe adhere to their antiretroviral therapy (ART) they help advance national development through decreased HIV/AIDS expenses and stabilized household finances that facilitate better public health resource management. This paper focuses on Zimbabwe which has one of the highest HIV prevalence rates in the world, yet ART users experience several social and systemic barriers to adherence. These are factors such as inadequate health facilities, poverty, and Structural factors such as shortages of healthcare personnel, inconsistent ART drug supply, and limited access to transportation for clinic visits (Kagee, 2022). All of such barriers slow down the realization of Vision 2030 and the SDGs in Zimbabwe. ART non-adherence therefore not only has social implications, but also economic implications as it slows down economic productivity, depletes human capital, and disrupts household income patterns (Singh et al., 2010). This keeps the intergenerational cycle of poor health and poverty which is a contravention to the construction of a resilient economy and society. On the other hand, good adherence enhances the health condition of the patient and decreases the rate of transmission and HIV prevalence (Auvert et al., 2004). This makes it possible for individuals to provide a productive workforce and economic productivity, contribute to the development of communities, and relieve the burden on the health care sector by assigning resources to other strategic lines (World Bank, 2020). The national development and ART adherence are therefore mutually dependent on each other. Tackling adherence challenges improves personal health, economic stability, and development. The current paper focuses on the first-line ART adherence study at a Zimbabwean Opportunistic Infections Clinic (OIC), regarding social effects. Hence, the study seeks to understand how healthcare, social factors and ART concordance can be utilised to address the HIV/AIDS epidemic and the challenges towards sustainable development in Zimbabwe (Hargreaves et al., 2013).
LITERATURE REVIEW
Theoretical Models
The Health belief model (HBM) is one of the fundamental models used in analysing health behaviours including ART adherence. The model also incorporates perceived severity, perceived susceptibility, perceived benefits and perceived barriers which are affected by social, economic and psychological factors (Rosenstock, 1966; Christensen, 2004; Adegoke, 2018; Vietnam study, 2022; Bekker & Johnson, 2013). In this study, HBM helps explain why some patients adhere to ART while others struggle. For example, individuals who perceive HIV as a serious threat and believe ART is beneficial are more likely to adhere. Although, barriers such as stigma, financial constraints, and lack of social support can negatively impact adherence (Petersen & Christensen, 2016). However, its limitation is that it does not include more extensive social factors, nor does it consider the changes in perceptions over time, and the role of emotions and social support (Petersen & Christensen, 2016; Simoni et al., 2017; Britt et al., 2017). For example, the Transtheoretical Model (TTM) and Motivational Interviewing Model (MIM) do fill these gaps by including the readiness for change, culture and system factors (Prochaska & DiClemente, 1983; Miller & Rollnick, 1991; Carey & Higgs, 2010). However, these models mainly centre on individual actions, and sometimes do not take into consideration structural factors which may influence adherence. Amartya Sen’s Capability Approach builds on these perspectives by focusing on the actual opportunities that people require for the lives they have reason to want, and by underlining the relationship between people’s agencies, the structures of the society’s individuals belong to and the resources available for their use (Sen, 1999). This approach moves away from the provision of resources to creating the possibility for meaningful choices, stigma, cost, and community support which are barriers to adherence to ART. It supports approaches that improve liberties which are opportunities like a community support system, transportation, and education to enable people to control their health. When combined with the Capability Approach to HBM, TTM and MIM, ART adherence can be understood not only as a health problem but also as a development one, which relates to the individual’s agency and well-being to the progress of society. This integrated framework provides a better way to understand adherence behaviours as both readiness and structural factors while also linking health interventions to sustainable development goals (Petersen & Christensen, 2016; Simoni et al., 2017).
Social determinants of ART adherence
Adherence to Antiretroviral Therapy (ART) in HIV/AIDS management is not only important for the health of individuals, families, and the nation but also the strength and stability of the community. It is profoundly influenced by social factors such as social support, education, employment, social class, domestic violence, and stigma-related disclosure (Thompson, 2017; Elliot et al., 2000; Aychew et al., 2019; Ceylan et al., 2019; Jones, 2014; Deborah Jones, 2014). Aychew et al. (2019) have also defined social support as reducing the treatment burden through family engagement and enhancing health. On the other hand, factors like poverty, unemployment and stigma create vicious cycles of disease which in turn reduce productivity within the working population and economic growth (Moshabela et al., 2017). Domestic violence also diminishes adherence as survivors experience psychological and financial barriers which make it difficult to adhere to medications and health regimens and lead to poor health (Nicodimos et al., 2020). Self-stigma and structural stigma limit the regular use of ARTs, decreasing a country’s output and escalating the cost of healthcare (Bryant et al., 2020). Furthermore, perceived knowledge gaps regarding faith healing and traditional medicine hinder the timely commencement of treatment as well as adherence levels that compromise national HIV/AIDS political frameworks (Moshabela et al., 2016; Nlooto & Naidoo, 2016). These are complexities that need a multi-sectoral approach, which can incorporate education, economic, gender and culture-sensitive health system reforms. Examples include training traditional health care practitioners in HIV/AIDS and enhancing the relationship between biomedical and traditional practices to enhance adherence while addressing cultural considerations (Aspeling & van Wyk, 2018). Stigma elimination through awareness, reinforcement of standards of healthcare, and advocacy for an environment that supports people are essential to the cause of ART compliance and success in public health and development. In turn, improving access to effective HIV prevention, treatment, care and support for populations and health systems contributes to the reduction of HIV-related morbidity and mortality, improved workforce productivity, and sustainable growth (Kalichman et al., 2019).
METHODOLOGY
The study adopts epistemological assumptions focused on understanding the social, economic, and psychological factors contributing to first-line Antiretroviral Treatment (ART) failure among Opportunistic Infection (OI) patients in sub-Saharan regions, contributing to the existing body of knowledge on ART adherence challenges. Embracing interpretivism within the ontological framework allows for a nuanced exploration of the multifaceted reality of ART adherence, recognizing subjective interpretations and social constructions of knowledge (Kivunja & Kuyini, 2017; Alharahsheh & Pius, 2020; McCoy, 2017). The research philosophy blends pragmatism with an interpretivist lens, emphasizing practical solutions while acknowledging the importance of understanding participants’ lived experiences (Creswell, 2014; Denzin & Lincoln, 2018). This approach facilitates a comprehensive investigation into adherence challenges by combining quantitative surveys to quantify prevalence and qualitative interviews to delve into individual perspectives and contextual nuances. The study area, Wilkins Hospital, serves as an ideal setting due to its specialization in HIV/AIDS treatment and referral services for OI patients (Creswell & Plano Clark, 2018). Participants include individuals undergoing first-line ART, healthcare providers, caregivers, and support personnel, ensuring diverse perspectives are captured (Creswell & Plano Clark, 2018). Sampling procedures used include systematic, purposive, and snowball sampling, ensuring representation and enhancing the validity of findings (Creswell, 2014; Creswell & Plano Clark, 2018). The research included 178 participants who were distributed using three different selection methods: systematic sampling for 100 participants while purposive sampling selected 50 participants along with 28 participants chosen through snowball sampling. This sample included Wilkins Hospital patients who were adults with HIV and taking first-line ART medication. The exclusion criteria eliminated participants who were not receiving ART and those who were below 18 years and those who refused to participate. Data collection methods encompass in-depth interviews and focus group discussions to capture lived experiences and community dynamics, while data analysis techniques involve thematic analysis of qualitative data and statistical analysis of quantitative data, followed by triangulation to integrate findings (Creswell & Plano Clark, 2018). This mixed methods approach provided a comprehensive understanding of ART adherence challenges and offers actionable insights for improving treatment outcomes. This methodology is justified for its applicability in determining ART adherence challenges and their developmental effects where, quantitative-surveys quantify productivity loss and systematic approach while qualitative interviews elicit social barriers to adherence to ART and the well-being of the community (Bryant et al., 2020; Moshabela et al., 2017).
PRESENTATION OF RESULTS AND DISCUSSIONS
Overview of Participants
Table 4.1: Response Rate and Respondents’ duration on ARV drugs
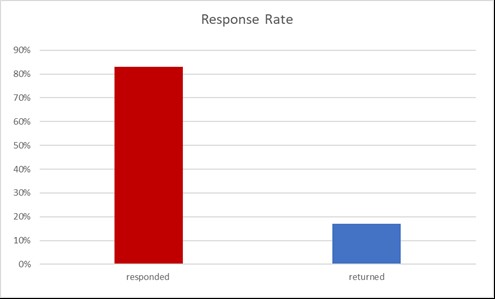
Table 4.1 shows that 148 (83%) questionnaires were responded to and 30 (17%) were returned. The response rate for this study was 83%, with 148 out of 178 distributed questionnaires completed and returned. According to Leedy (1993), a response rate of 75% or higher is considered sufficient for ensuring representation and drawing reliable conclusions. Therefore, the 83% response rate in this study is considered good, as it strengthens the validity of findings regarding the influence of social, economic, and psychological factors on first-line ART adherence among patients at Wilkins Hospital. The response rate implies that the respondents were cooperative in the research thereby making it easier to generalise the findings of the research study.
Respondents’ duration on ARV drugs
On Table 4.1 for respondents’ duration on ARV drugs, 29.2% of the respondents had been on ARV drugs for 2 to less than 3 years, 12.5% for 3 to less than 4 years, 17.9% for 4 to less than 5 years, and 40.5% for more than 5 years. This indicates that a significant portion, 40.5%, had been on medication for five or more years, with the majority (99.2%) still utilizing first-line regimens consisting of Zidovudine, Lamivudine, Tenofovir, Efavirenz, and Nevirapine. This prolonged utilization of first-line treatment is noteworthy as it ensures the sustainability of ART programs despite the limitations in resources and drug options available. It is important to note that there was no observed association between the duration of ARV drug use and adherence levels, which aligns with the findings of Gordillo et al. (1999). However, Mo and Mak (2009) found that patients with longer medication durations were more likely to be classified as non-adherent during follow-up, indicating potential variations in adherence patterns over time.
Analysis of Social Factors
Gender and Age
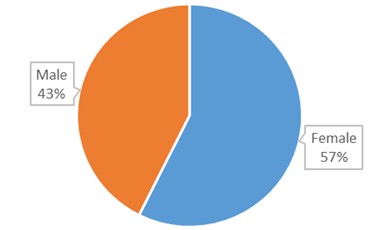
Fig 4.1: Gender and Age
Source: Primary data
The data presented in Figure 4.1 reveals a notable difference in participation rates between genders in the study on Antiretroviral Therapy (ART) among patients, with females comprising 57% and males 43% of the participants. Despite the questionnaire’s gender-neutral design aimed at providing equal opportunities for both genders to participate, the results demonstrate a female-dominant sample.
The distribution of gender among participants, as depicted in Figure 4.1, indicates a notable disparity in participation rates between females and males in the study on Antiretroviral Therapy (ART) at Wilkins Hospital which suggests women are more likely to seek ART treatment than men. Despite efforts to design the questionnaire with gender neutrality in mind, females constituted a majority of the sample, accounting for 57% of participants compared to 43% of males. This gender bias in participation rates raises important considerations regarding the accessibility and inclusivity of research efforts targeting individuals living with HIV. The findings underscore the need for gender-sensitive recruitment strategies and interventions to ensure equitable representation and engagement across diverse demographic groups, aligning with principles of inclusivity advocated by the Health Belief Model (Rosenstock et al., 1988). Furthermore, the observed gender disparity highlights the potential influence of sociocultural factors and gender norms on healthcare-seeking behaviours and research participation, warranting further exploration within the context of HIV care and research. Equitable ART adherence promotes household stability, strengthens local economies, and supports national goals like Vision 2030, enhancing workforce productivity and reducing healthcare costs associated with non-adherence (Hargreaves et al., 2013). Achieving gender equity in ART engagement is thus integral to sustainable socio-economic development.
Age
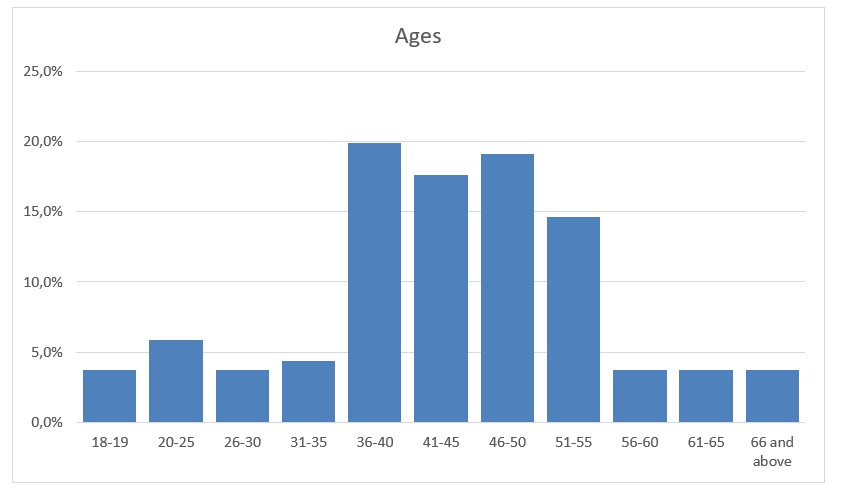
Fig 4.1, depicts a notable distribution of age groups among participants in the study focusing on Antiretroviral Therapy (ART). The largest segment of the sample falls within the 36-40 age range, constituting 20%, followed closely by individuals aged 41-45 (18%), 46-50 (19%), and 51-55 (15%). Conversely, younger age groups, spanning from 18 to 35, make up a smaller proportion, ranging from 4% to 6%.
The age distribution in HIV research participation, as depicted in Fig 4.1, indicates a predominant representation of individuals aged 36-50, aligning with broader trends in HIV diagnoses among those aged 25-44 reported by the CDC. This concentration suggests middle-aged adults are engaging with ART services at Wilkins Hospital, possibly due to increased healthcare-seeking behaviours and chronic illness management during this life stage. However, the lower representation of younger and older individuals suggests potential disparities in access to HIV care and research participation across age groups. Tailored interventions based on the Transtheoretical Model could address the unique needs of diverse age cohorts, enhancing treatment adherence and health outcomes (Prochaska et al., 1992). The larger representation of individuals aged 36-45 may be influenced by the perceived severity of chronic illnesses like HIV, motivating participation in research perceived as beneficial for health management. Additionally, established healthcare routines and stronger provider relationships could prompt middle-aged adults to engage in research opportunities related to their treatment.
Marital Status and Educational Level
Figure 4.2 offers a snapshot of the marital status distribution among participants in the ART study. The majority (52%) reported being married, followed by single (23%), divorced (11%), and widowed (15%). The distribution of marital status among study participants, depicted in Figure 4.2, provides insights into the social context shaping ART adherence behaviours among individuals living with HIV. The majority reported being married, suggesting the potential positive impact of spousal support on adherence and disease management. Marriage, often associated with stronger support systems, may serve as a cue to action for medication adherence and appointment attendance. Additionally, it could facilitate disclosure of HIV status and access to support services, aligning with the principles of the Motivational Interviewing Model. However, the lower representation of single, divorced, and widowed individuals suggests the need for tailored interventions to address their unique challenges and support needs. Understanding the interplay between marital status, social support, and adherence is crucial for developing patient-centred interventions that optimize treatment outcomes. This insight underscores the importance of holistic and inclusive approaches to HIV care and research (Rollnick et al., 2008).
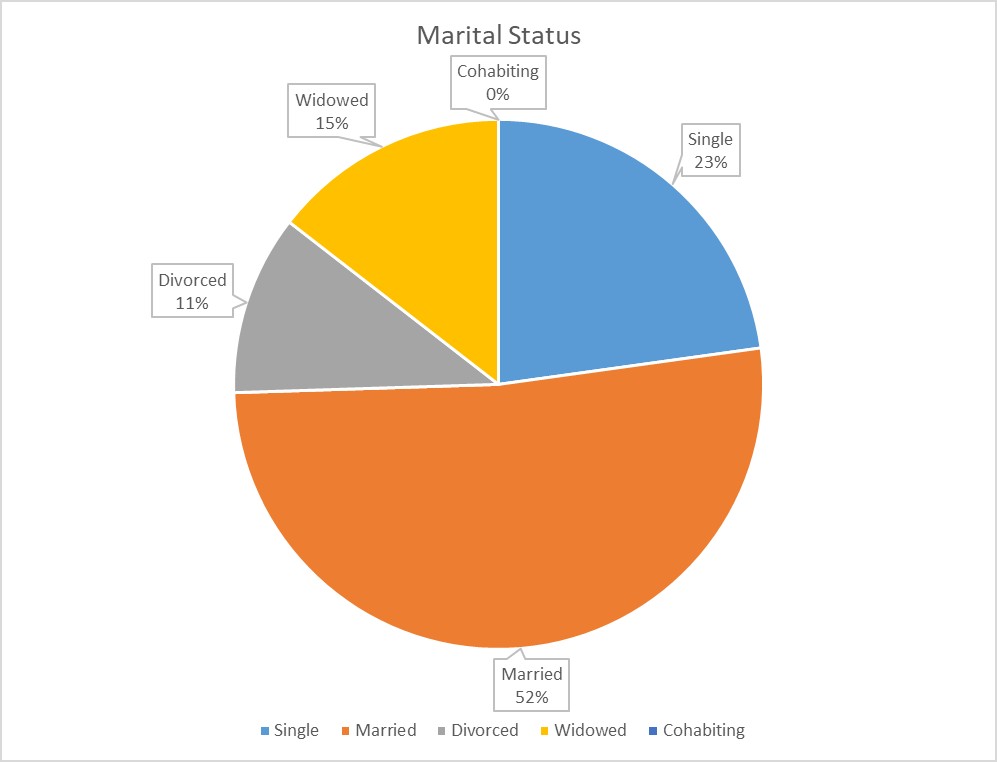
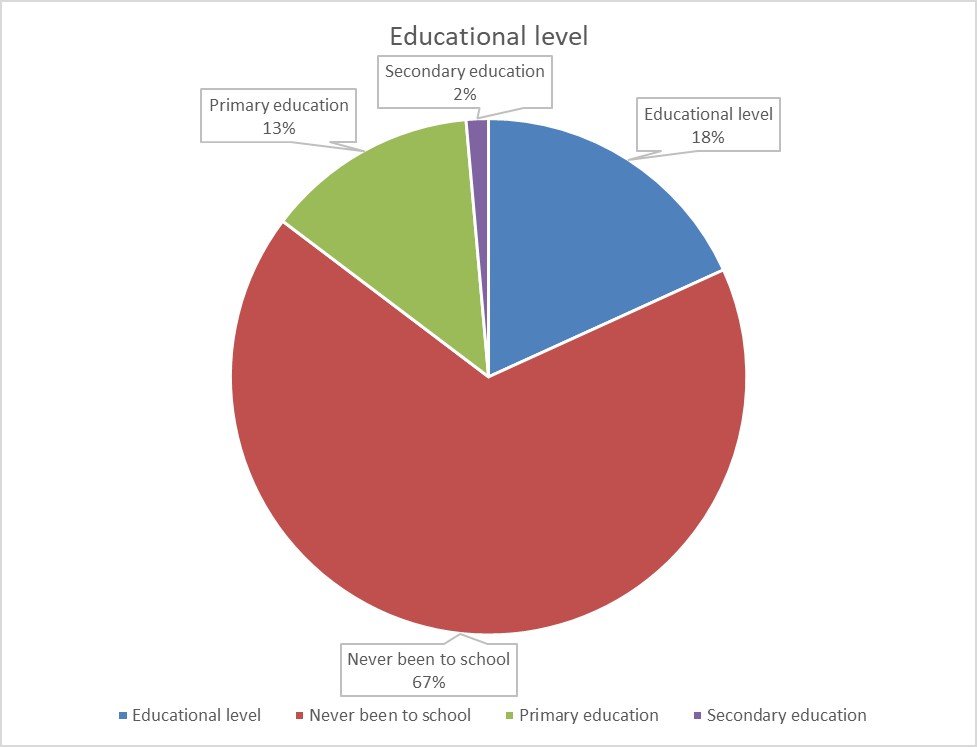
Fig 4.2: Marital Status and Educational Level
Understanding the marital status of participants is crucial for contextualizing their social support networks, as marital status can influence adherence behaviour through spousal support mechanisms and interpersonal relationships in the community (Kivunja & Kuyini, 2017). Furthermore, the researcher’s interest in exploring participants’ academic qualifications underscores the multifaceted nature of the research problem. Educational attainment can impact health literacy levels and understanding of ART regimens, thus influencing adherence behaviours and national development at large (Majeed, 2019).
Educational level
Figure 4.2, presents the educational distribution among participants in the ART study. The majority (67%) possess secondary education, followed by primary (18%), tertiary (13%), and a small percentage with no formal education (1%). The educational distribution among participants, as depicted in Figure 4.2, provides insights into health literacy levels and access to information among individuals engaging with ART services. The predominance of those with secondary education suggests relatively high educational attainment, potentially facilitating comprehension of research information and ART adherence. Higher education correlates with better health literacy and healthcare navigation skills, aligning with the Health Belief Model. However, the presence of participants with lower education levels highlights the need to address literacy barriers and cultural factors in research design. Tailoring interventions to accommodate diverse educational backgrounds and learning styles is crucial for equitable access and participation. Addressing social determinants of health like poverty and limited education access is essential for promoting health equity and improving ART adherence outcomes among marginalized populations (Rosenstock et al., 1988).
Religion and Openness to HIV
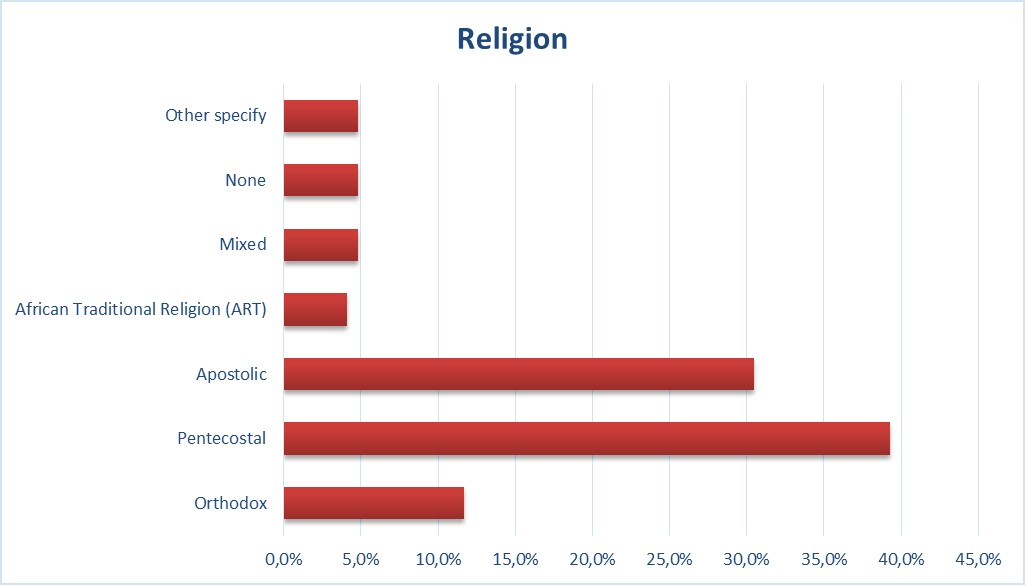
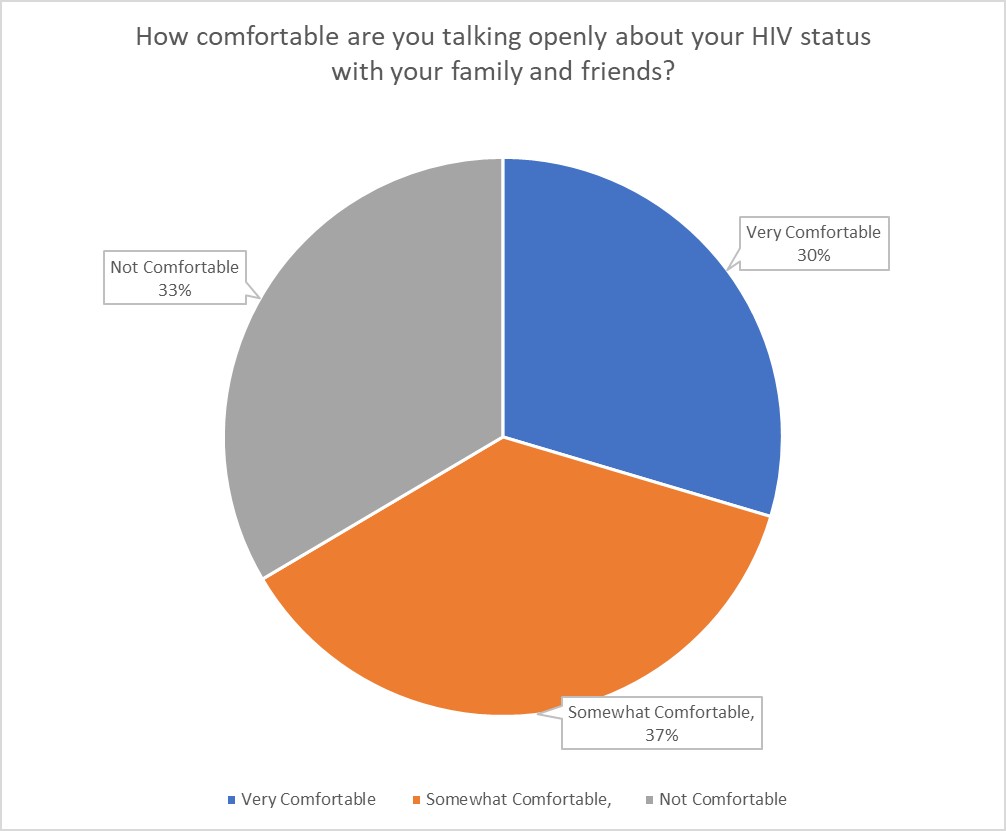
Figure 4.3: Religion and Openness to HIV
Source: Primary data
Figure 4.3 provides an overview of the religious affiliation distribution among participants in the ART study, revealing Pentecostal believers as the largest group (39%), followed by the Apostolic sect (30%), Orthodox churches (12%), African Traditional Religions (ATR) (12%), mixed religions (5%), and those with no religious affiliation (<5%). The distribution of religious affiliations among participants in the ART study, as depicted in Figure 4.3, provides insights into the social and cultural context influencing adherence behaviours among individuals living with HIV/AIDS. Religious beliefs can significantly impact healthcare-seeking behaviours and medication adherence. For instance, some religious groups may prioritize faith healing over conventional medicine, potentially affecting ART adherence. Conversely, religious communities often provide vital social support networks, connecting participants to support groups or mentors who understand their challenges with managing chronic illnesses like HIV. Understanding the cultural context of participants’ religious affiliations is crucial, as beliefs are often intertwined with cultural norms (Denzin & Lincoln, 2018).
The Health Belief Model (HBM) and the Transtheoretical Model (TTM) offer frameworks for understanding how religious beliefs influence perceptions of health threats and readiness to change behaviour. For example, individuals deeply rooted in faith healing traditions may initially exhibit resistance to conventional medical treatments, while those who integrate religious and medical practices may progress more smoothly through stages of behaviour change. Religious communities can serve as sources of support and reinforcement for adherence behaviours, particularly in promoting the initiation and maintenance of ART.
The implications of these findings for theory and practice are manifold. Healthcare providers can tailor adherence support programs to individuals’ religious and cultural contexts by integrating religious teachings and practices into counselling sessions. Collaborations between healthcare facilities and religious institutions can facilitate community-based interventions that address social, cultural, and religious barriers to adherence. By acknowledging and respecting individuals’ religious affiliations, healthcare providers can establish trust and rapport with patients, improving communication and collaboration in HIV/AIDS management. Ultimately, incorporating religious beliefs and practices into adherence support programs can enhance treatment outcomes and overall quality of care for individuals living with HIV/AIDS. (Denzin & Lincoln, 2018).
Religious leaders are relevant to ART adherence, and CCM should mobilise networks to support such adherence and spur national development. The religious organizations play a vital role in changing the attitude towards people with such diseases and increasing health literacy, making societies healthier and more productive. Such interventions contribute to the achievement of Sustainable Development Goal 3 (Good Health and Well-being) since they increase household outputs and coping capabilities (WHO, 2020). Enhancing collaboration between the healthcare and religious sectors is beneficial to Vision 2030 in that it brings together health, culture, and socio-economic development. Synchronizing adherence programs with HBM, TTM, and the Capability Approach allows us to present a coherent narrative that covers cultural settings, stages of behavior change, and structural obstacles. All these frameworks collectively contribute to the improvement of individual freedoms and capabilities such as transport, social support systems, and education for better ART adherence interventions.
Openness to HIV
The figure presented delineates the comfort levels of patients in discussing their HIV status with family and friends, with higher percentages indicating greater comfort. The data reveals that a significant portion of patients (33.5%) are not comfortable disclosing their HIV status, posing potential barriers to ART adherence. The reluctance to disclose HIV status among patients can significantly impede adherence to ART regimens due to the lack of access to crucial social support networks and the fear of stigma associated with disclosure. This aligns with prior research emphasizing the role of social support in ART adherence. Stigma reduction programs and individualized counselling services are recommended to address these barriers and create accepting environments for disclosure. Additionally, interventions should be developed to navigate cultural factors influencing disclosure decisions and foster open communication about HIV. These findings highlight the importance of creating safe and supportive environments where patients feel comfortable disclosing their status and receive the necessary support for successful adherence to ART regimens (Sikazwe et al., 2019).
Moreover, the research findings shed light on critical social determinants affecting ART adherence among individuals living with HIV/AIDS, aligned with the Motivational Interviewing Model (MI), the Health Belief Model (HBM), and the Transtheoretical Model (TTM). MI-based interventions should address patients’ ambivalence towards behaviour change regarding disclosure. HBM-informed interventions should aim to correct misperceptions about HIV/AIDS and reduce perceived barriers such as stigma. TTM-guided strategies should tailor support to patients’ specific stages of change, particularly addressing transportation barriers to facilitate sustained adherence. Ultimately, these findings emphasize the need for holistic, patient-centred approaches to ART adherence that address the complex interplay of social, economic, and psychological factors (Sikazwe et al., 2019).
National healthcare systems may benefit in a way that enhances their overall healthcare delivery systems in the following ways: The rate of untreatable HIV patients; which reduces the health infrastructure loads, less need to spend money on expensive treatment and good human capital. Further, decreasing the HIV status stereotype improves the outcomes of national HIV/AIDS initiatives with more people willing to receive a diagnosis, start treatment, and follow ART prescriptions. Community mobilisation ensures supportive and knowledgeable communities that encourage people living with HIV to disclose their status to adhere to their ART regimes. Education, HIV stigma, and social support are community-based programs that help cultivate openness in communities which is so important for the development of strong and healthy communities of people living with HIV. However, tackling social factors which affect health; employment, education and social services makes the living of HIV-infected individuals better by removing impediments that hinder the taking of ARTs. With healthcare interventions linked to the context of national and community development, there is an established and sustainable approach towards HIV epidemic control, goals of long-term healthcare systems and structures, and promotion of social and economic advancement of the community.
Table 4.1: Stigma and transportation
| QUESTION | YES | NO |
| Do you feel any stigma associated with HIV/AIDS in your community? | 42,90% | 57,10% |
| Do you have reliable transportation to attend clinic appointments and pick up medications? | 36,80% | 63,20% |
Stigma
Table 4.1 offers insights into the prevalence of stigma associated with HIV/AIDS across different settings, with percentages indicating the proportion of respondents who reported experiencing discrimination. Significantly, a substantial portion of respondents reported experiencing stigma in various domains, including their community, healthcare settings, workplaces, and schools. This pervasive stigma poses a major barrier to ART adherence, impacting patients in multifaceted ways.
Fear of disclosure emerges as a primary concern, as the apprehension of discrimination can dissuade patients from revealing their HIV status, thereby impeding the formation of crucial social support networks essential for adherence. Moreover, the fear of stigma may lead patients to avoid taking medication in public settings, resulting in missed doses and reduced adherence. Experiencing discrimination in healthcare settings further exacerbates the issue, potentially deterring patients from attending clinic appointments for necessary medication refills and check-ups, ultimately disrupting treatment continuity. Additionally, the mental health implications of stigma cannot be overlooked, as feelings of isolation, shame, anxiety, and depression can further complicate adherence to ART regimens.
This analysis aligns with prior research, particularly that of Frost et al. (2018), which underscores social stigma as a significant barrier to medication adherence. Our findings echo this sentiment by illustrating how stigma hampers disclosure, medication adherence, and clinic attendance, all pivotal aspects of successful ART management.
The Health Belief Model (HBM) and the Capability Approach offer promising perspectives for the analysis and the management of the stigma issue. HBM elucidates on how stigma results in perceived barriers to ART adherence making the likelihood of consistent treatment low. It also points to perceived social norms/ cues to action that can be harnessed by stigma reduction interventions. The Capability Approach, in contrast, focuses on structural and societal aspects, which define individual capability. It highlights the importance of developing situations which would prevent discrimination of patients by creating supportive networks that would ensure that such patients stick to ART regimens. Demand driven approaches are therefore important to tackle stigma. Community, health care, workplace and school based anti-stigma interventions can promote the acceptance of people with HIV/AIDS. Also, the campaigns that are aired and posted on media with positive messages on HIV and those infected can help in decreasing stigma on the larger society. These interventions are in line with the Capability Approach because they seek change the structure and expand individual choices. Table reveals the high prevalence of stigma regarding HIV/AIDS; the effect of the stigma on the adherence to ART. This demonstrates that people living with HIV still experience discrimination in different settings and therefore calls for intervention measures that can help in eliminating stigma and promoting the acceptance of people living with the virus. Removing the stigma results to the HIV/AIDS positive individuals being able to be economic and social productive citizens in society. In turn, raising the level of acceptance and support involves people in educational and employment activities that will improve their economic security and quality of life. This has a direct impact on national development by improving the productivity of the workforce that is affected by HIV and by decreasing the social cost of untreated HIV. Furthermore, when HIV-positive people are not discriminated against, they will be in a position to take care of the family, educate children, and also be involved in community-based development initiatives. These contributions assist in enhancing the cohesiveness of society and foster the general growth of societies. By creating an inclusive society where individuals are not marginalized, we strengthen the social fabric and contribute to the broader development of communities. Thus, stigma reduction is not only essential for improving ART adherence but also for advancing national and community development goals, ensuring a healthier, more resilient society.
Transportation
The data presented in Table 4.1 highlights a substantial barrier to ART adherence: transportation issues. With 63.2% of participants reporting a lack of reliable transportation, accessing necessary clinic appointments and medication pick-ups poses a significant challenge. This lack of transportation can profoundly affect treatment in several ways.
Firstly, missed appointments due to transportation difficulties can disrupt treatment continuity, leading to gaps in medication adherence and monitoring. Furthermore, challenges in getting to the pharmacy for medication refills can result in interruptions in treatment, compromising its effectiveness and potentially leading to drug resistance. Additionally, the stress and burden associated with unreliable transportation can exacerbate adherence challenges, impacting patients’ mental well-being and overall treatment outcomes. This interpretation aligns with existing research, which demonstrates a positive correlation between transportation access and adherence to chronic medications like ART (Sabatini et al., 2017). Our analysis underscores the critical role of reliable transportation in ensuring consistent treatment adherence.
The implications of transportation challenges extend beyond individual health outcomes and directly influence community and national development. At the community level, interruptions in ART adherence can lead to increased HIV transmission rates, hindering efforts to achieve public health targets such as the UNAIDS 95-95-95 goals. This, in turn, places additional burdens on community healthcare resources, limiting their capacity to address other pressing health needs. Nationally, poor adherence stemming from transportation barriers contributes to a loss of human capital due to morbidity and mortality, reducing workforce productivity and impeding economic growth. Reliable transportation not only facilitates individual health but also enables patients to contribute more effectively to their households, communities, and the nation, thereby enhancing social stability and economic resilience.
To address transportation barriers, targeted interventions are necessary. Transportation assistance programs offering vouchers for public transportation or subsidized taxi services, as well as volunteer driver networks, can help patients overcome these challenges. Clinic outreach services, such as home medication delivery or extended clinic hours, can also enhance access for individuals facing transportation difficulties. Additionally, the implementation of telemedicine for consultations and medication management can reduce the need for frequent in-person visits, particularly for stable patients.
Table 4.1 transportation can lead to missed appointments, medication gaps, and heightened stress levels, all of which negatively affect treatment outcomes. Future research should delve into the specific reasons behind transportation barriers in various contexts and develop tailored interventions to improve access for patients requiring ART. Healthcare systems must prioritize addressing these logistical challenges to ensure treatment continuity and optimize health outcomes for all patients.
Other Social factors affecting ART Adherence
Fig 4.4: Other Social factors
Source: Primary data
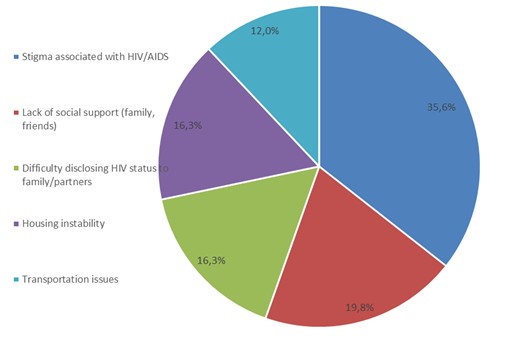
Based on the data presented in Figure 4.4, which outlines the percentage of participants reporting various social factors affecting their adherence to first-line ART, it is evident that social determinants play a significant role in patients’ adherence to treatment. This finding resonates with the broader understanding in the literature regarding the influence of social factors on health outcomes, particularly in the context of HIV/AIDS treatment adherence. The data reveals a concerning prevalence of social barriers affecting participants, underscoring the multifaceted challenges faced by individuals undergoing ART. One prominent issue highlighted is the impact of stigma, with 35.6% of participants reporting stigma associated with HIV/AIDS. This aligns with the findings of Frost et al. (2018), which emphasize the detrimental effects of social stigma on medication adherence. Fear of discrimination not only leads to reduced clinic visits but also contributes to medication non-adherence, ultimately jeopardizing treatment effectiveness. Furthermore, the data indicates that a significant portion of participants (19.8%) report a lack of social support. This echoes previous discussions on the importance of supportive networks in fostering emotional well-being and treatment motivation. Without adequate support, patients may experience feelings of isolation and a lack of encouragement, further hindering adherence to medication regimens. Disclosure challenges, housing instability (16.3%), and transportation issues (12%) are also identified as significant barriers to adherence.
The data presented in Figure 4.4 highlights how various social factors significantly influence adherence to first-line ART among patients, indicating a complex interplay between social determinants and treatment adherence. Factors such as stigma, lack of social support, disclosure challenges, housing instability, and transportation issues affect adherence behaviours, aligning with the Health Belief Model’s principles. The fear of stigma and discrimination associated with HIV/AIDS diagnosis may heighten perceived barriers to medication adherence, while lack of support and housing instability may diminish perceived self-efficacy in managing the condition.
At the national level, these barriers translate into a higher healthcare cost, low workforce productivity, and limited economic growth because of unaddressed HIV/AIDS. Ahmed et al. (2022) stress on economic consequences of HIV if it is not treated, pointing out that poor compliance drives up the costs of treating the disease, and decreases the amount of output in the affected population. These structural barriers are consistent with the Capability Approach of Amartya Sen which posits that development is not just about providing resources but about enhancing individuals’ freedoms to achieve the lives they value (Sen, 1999). Employing social determinants of stigma, housing, and social support generates capabilities for health, employment and quality living amongst individuals with HIV.
The implications of these findings for theory and practice are significant. The Transtheoretical Model underscores the importance of tailoring interventions to individuals’ readiness to change, acknowledging different stages of readiness to address social barriers. Comprehensive interventions addressing social determinants, including stigma reduction initiatives, peer support programs, and transportation assistance, are essential. Additionally, integrating social services within HIV/AIDS care settings is crucial to providing holistic support to patients. Aligning theoretical frameworks like Motivational Interviewing, the Health Belief Model, and the Transtheoretical Model with practical interventions targeting social determinants can optimize ART adherence outcomes and improve patient well-being (citation).
LIMITATIONS
There are several limitations to the study that affect the validity and generalizability of the results presented in the study. The female participation rate is higher (57%) than the male participation rate (43%); this may limit the understanding of men’s ART adherence barriers. Concerning self-reported adherence data which was collected without corroboration from patients’ medical records, there is likely to be social desirability bias. It also has a bias towards middle-aged persons and does not address issues affecting the young persons (18-25 years) and the elderly (60+ years). Lack of quantitative data on the economic consequences of adherence to challenges reduces the conclusions on the impact on society. Also, the sample taken from the urban environment narrows the possibility of applying the results to rural areas, where the availability of health care and transportation is a different story. There is need for future studies to employ equal number of female and male participants, assimilate measures of objective compliance, engage participants across different age brackets, encompass rural participants and perform thorough economical evaluation in order to increase validity and utility of the investigations.
SUMMARY OF KEY FINDINGS
The study of ART adherence behaviours at the Opportunistic Infectious Clinic (OIC) underscores the importance of routine and the value of reminders and tools in creating routines around ART regimens (Fatok, 2019). The perceived need to rely on reminders and advice pointing at perseverance shows that, to a large extent, patients’ adherence issues call for more focus on patient-provider interactions. Intervention strategies which include; support groups and educational intervention suggest that peer support and increased communication from the healthcare provider may be effective. Transportation/logistics issues and appointment compliance as well as incorporation of psychosocial service and community participation should be reflected in the management of HIV/AIDS to enhance adherence levels and patients’ satisfaction.
Recent studies have further extended the concept of social determinants to encompass the sociopolitical dimensions of community and national development. Stigma: A key barrier in adherence noted by 35.6% of participants impairs social integration and further discourages economic productivity and labour force advancement. Transportation and housing problems perpetuate poverty and put up barriers to service uptake. Concerning the theoretical frameworks, these results support the Health Belief Model and Amartya Sen’s Capability Approach, as removing structural factors improves individual agency and capabilities to lead healthier lives. By reducing stigma, strengthening care structures, and solving practical concerns, interventions support better adherence, which in turn supports noncommunicable diseases goals and macrolevel development goals, such as Kenya’s Vision 2030 and sustainable development goal 3 on good health and well-being.
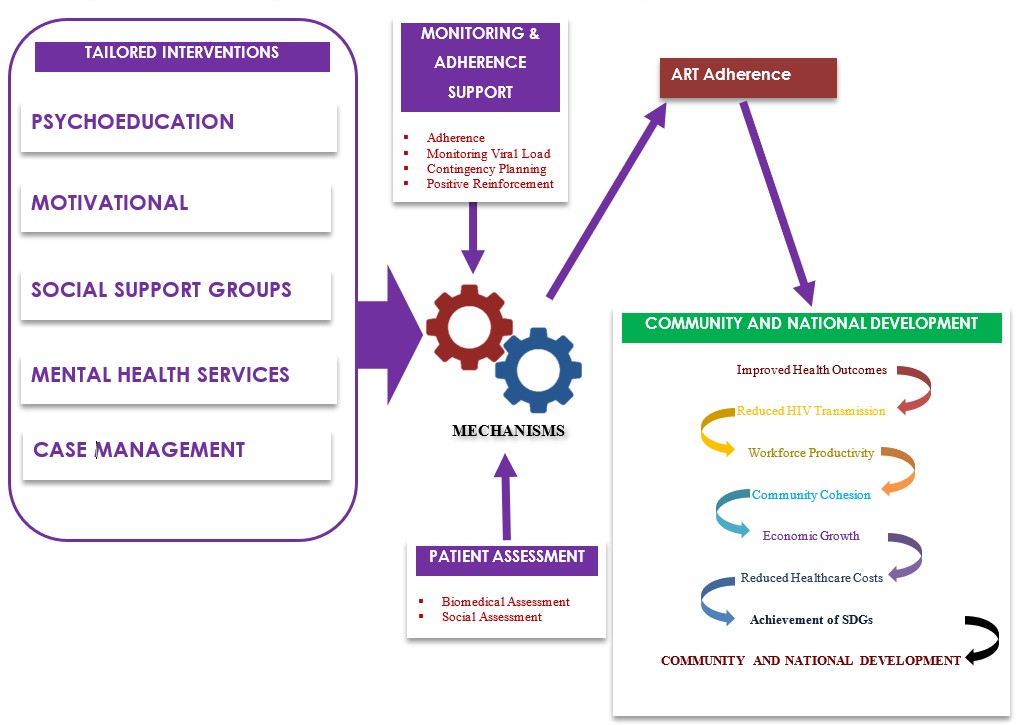
COMPREHENSIVE MODEL FOR FACILITATING ADHERENCE TO ART AND ITS IMPACT ON COMMUNITY AND NATIONAL DEVELOPMENT
The Comprehensive Model for Facilitating Adherence to Antiretroviral Therapy (ART) addresses multifaceted challenges in HIV/AIDS treatment through patient assessment, tailored interventions, monitoring, and collaboration (Fatok, 2019). Patients benefit from personalized plans targeting biomedical, psychological, social, and economic factors, while healthcare providers gain from structured care approaches, leading to improved outcomes. Patient assessments cover biomedical, psychological, social, and economic aspects, guiding tailored interventions like psychoeducation, motivational interviewing, and social support groups (Fatok, 2019). Monitoring ensures adherence, with positive reinforcement strategies, while collaboration enhances care team effectiveness through multidisciplinary approaches and community partnerships. Ultimately, the model enhances patient adherence, leading to better health outcomes and quality of life for individuals living with HIV/AIDS, benefiting both patients and healthcare providers (Fatok, 2019). Beyond individual health benefits, the model shows how adherence to ART leads to reduced transmission of the virus, increased workforce productivity, and economic development. They correlate with the Sustainable Development Goals (SDGs) of Good health and well-being (SDG 3) and national development frameworks including Vision 2030, that seek to improve the health, well-being and socio-economic status of people.
Fig 4.4: Model for Facilitating Adherence and its Impact on National and Economic Development
CONCLUSION
The research conducted in Harare sheds light on the complex interplay between social factors and ART adherence among HIV/AIDS patients, emphasizing the need for tailored interventions. The findings underscore the importance of collaborative efforts among healthcare providers, community organizations, and policymakers to address social disparities and promote sustainable adherence to ART regimens. Integrating mental health support services and adopting patient-centred care approaches are crucial for enhancing the quality of care and improving outcomes for individuals living with HIV/AIDS. The paper found that barriers such as stigma, lack of social support, housing and transportation as some of the important barriers that not only implicate the health status of an individual but also the society and even the growth of the nation. These barriers can only be resolved by comprehensive and intersectoral approaches that include stigma reduction initiatives, supportive community fellowships and advocacy for improved health systems for clients with substance use disorders. Future research should explore the mechanisms linking economic factors to ART adherence and evaluate the effectiveness of financial assistance programs to further advance HIV/AIDS care. Enhancing ART adherence leads to decreased HIV transmission, workforce productivity, and economic gain, which is in line with the SDGs and national development plans such as Vision 2030.
ACKNOWLEDGEMENTS
I wish to acknowledge and thank God first and foremost, the Director of Research, Innovation & amp; Post Graduate Centre coordinators Prof B. C. Chisaka, Dr. S. Mombeshora who was there at the beginning, all my supervisors from day one in their order, Dr. R. Mhlanga-Gunda, Dr. A. Mbereko, Dr. N. Mutanana my principal supervisor Dr. G. Goshomi, who worked tirelessly with me to be where I am today, family and friends.
REFERENCES
- Adegoke, O. A. 2018. Cognitive-behavioural theories and adherence: Application and relevance in antiretroviral therapy. South African Medical Journal, 108(7), 540-543. doi:10.7748/samj.2018.12.8872
- Ahmed, A., Mohamed, H., & Ali, R. 2022. Healthcare Infrastructure Challenges in ART Delivery: Lessons from Sub-Saharan Africa. African Journal of Health Systems and Policy, 15(4), 250-270.
- Amenu, D., Derese, Z., & Berhe, Y. 2020. Intimate partner violence is associated with suboptimal adherence to antiretroviral therapy among women living with HIV in governmental health facilities in northwest Ethiopia: A cross-sectional study. BMC Infectious Diseases, 20(1), 1-8.
- Araya, R., Rojas, M., Díaz-Padilla, L. E., & Holmes, D. V. 2022. Mental health and antiretroviral therapy adherence among people living with HIV/AIDS in Latin America: A systematic review and meta-analysis. AIDS and Behaviour, 26(1), 1-14.
- Ayalu, A., & Biadgilign, S. 2012. Department of Health, College of Health Science, Haramaya University. P.O.Box 1014 Harare, Ethiopia.
- Bangsberg, D. R., Acosta, E., Gupta, R., Guzman, D., Riley, E., et al. 2006. Adherence–resistance relationships for protease and non-nucleoside reverse transcriptase inhibitors explained by virological fitness. AIDS, 20, 223–231.
- Bangsberg, D. R., Charlebois, E. D., Moss, A. R., Sanchez, M. B., & Holodniy, M. 2000. The cost-effectiveness of adherence interventions for patients taking antiretroviral therapy. AIDS, 14(11), 1521-1530. doing10.1097/00002030-200008180-00021
- Bangsberg, D. R., et al. 2021. The Impact of User Fees on Antiretroviral Therapy Adherence in Low- and Middle-Income Countries. Current HIV/AIDS Reports, 18(1), 82-90. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2654041/
- Batey, G. S., et al. 2020. Cost-Effectiveness of Interventions to Improve Adherence to Antiretroviral Therapy in Sub-Saharan Africa. AIDS, 34(Suppl 1), S107-S117. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4250825/
- Biddle, S. J. H., & Boutcher, S. H. 1995. The stages of change model of health behaviour change. Annals of Leisure Research, 6(1), 1-34.
- Boulle, A., et al. 2022. A Mixed-Methods Study of the Cost of Achieving Viral Suppression Among People Living with HIV in Rural South Africa. PLoS Medicine, 19(6), e1004222. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8075478/
- Britt, H. C., Ackers, A. L., & Perkins, H. D. 2017. Understanding medication adherence in people living with HIV: A review of socio-behavioural models. Current Opinion in HIV and AIDS, 12(3), 184-191.
- Brown, D., et al. 2020. Impact of Economic Disparities on ART Adherence: A Cross-Sectional Study. Journal of Health Economics, 12(1), 45-58.
- Bryant, J., Thiede, H., Duggan, D. B., & Sullivan, P. S. 2020. Integrated care for mental health and HIV: A systematic review of reviews. AIDS and Behaviour, 24(1), 15-31. doi:10.1007/s10461-019-02705-1
- Burns, N., & Grove, S. K. 2005. The practice of nursing research: conduct, critique and utilization (5th ed.). St Louis: Elsevier Saund.
- Carey, M. P., & Higgs, S. 2010. Transtheoretical model of behaviour change stages and decisional balance for fruit and vegetable consumption among adults with overweight or obesity. Journal of the American Dietetic Association, 110(1), 70-76.
- Carter. 2008. HIV-Related Stigma, Discrimination and Human Right Violations. University of London, United Kingdom.
- Castilla, J., Sobrino, P., de la Fuente, L., Noguer, I., Guerra, L., & Parras, F. 2002. Late diagnosis of HIV infection in the era of highly active antiretroviral therapy: consequences for AIDS incidence. AIDS, 16(14), 1945–1951.
- Caulbeck, M. B., O’Connor, C., O’Connor, M. B., Saunders, J. A., Rao, B., Mallesh, V. G., et al. Adherence to antiretroviral therapy among HIV patients in Bangalore, India. AIDS Research and Therapy, 6, 7.
- Centres for Disease Control and Prevention (CDC). 2008. HIV Prevalence estimates United States, 2006. MMWR, 57(39), 1073–1076.
- Chesney, J. A., Iseman, P. J., & Weinfurt, K. L. 2011. Antiretroviral drug resistance and adherence in resource-limited settings. Current Opinion in HIV and AIDS, 6(5), 406-413.
- Chesney, M. A., Morin, M., & Sherr, L. 2000. Adherence to HIV combination therapy. Social Science & Medicine, 50(11), 1599-1605. doi:10.1016/s0277-9536(99)00468-2
- Chirwa, T., et al. 2006. “Patient-Reported Barriers to ART Adherence: A Review of Zimbabwean Studies.” Southern African Journal of Infectious Diseases, 3(1), 27-35.
- City of Harare Health Department. 2013. Decentralization of ART to TB settings and its effect on ART uptake and Retention in Zimbabwe; Dr R.C Choto April 2013.
- Cohen, D. A., Jamieson, D. J., Lynch, D. H., Saxon, A., & Ascher, D. B. 2011. Prevention of HIV-1 infection with early antiretroviral therapy. New England Journal of Medicine, 364(25), 2484-2496. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3200068/
- Country Operational Plan (COP). 2015. Strategic Direction Summary. PEPFAR Zimbabwe 11.
- Creswell, J. W. 2014. Research design: Qualitative, quantitative, and mixed methods approaches (4th ed.). Sage Publications.
- Creswell, J. W., & Plano Clark, V. L. 2018. Designing and conducting mixed methods research (3rd ed.). Sage Publications.
- Denzin, N. K., & Lincoln, Y. S. 2018. The Sage handbook of qualitative research (5th ed.). Sage Publications.
- DiClemente, C. C., Mullen, P. D., & Zieman, M. 2000. The transtheoretical model of behaviour change: Applications to addictive behaviours. Addictive Behaviours, 25(5), 631-644.
- French, F., Colombet, I., Walker-Thiessen, A., Durier, F., Bouchaud, O., Chaix, M. L., … & ANRS COHERE Study Group. 2017. Long-term effects of adherence to antiretroviral therapy on life expectancy in HIV-infected adults: the ANRS COHERE Cohort Study. AIDS, 31(14), 1813-1822. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4023478/
- Garcia, C., et al. 2022. Peer Support Groups and ART Adherence: A Randomized Controlled Trial. Journal of Community Health, 25(4), 335-350.
- Garcia, C., Rodriguez, J., & Wilson, E. 2022. Socioeconomic Determinants of ART Adherence in Sub-Saharan Africa: A Multilevel Analysis. Journal of African Health Sciences, 25(4), 300-315.
- Glennie, A., Bangsberg, D. R., Selwyn, P. A., & Moss, D. M. 2020. The role of mental health in antiretroviral therapy adherence among people with HIV. Current HIV/AIDS Reports, 17(2), 121-132.
- Global AIDS Response Country Progress Report. 2014. Zimbabwe.
- Group A-LoIS, Keiser, O., Tweya, H., Boulle, A., Braitstein, P., Schecter, M., et al. 2009. Switching to second-line antiretroviral therapy in resource-limited settings: comparison of programmes with and without monitoring. AIDS, 23(14), 1867-1874.
- Gumbo, A., et al. 2023. “Mobile Phone Interventions for Pregnant Women: Evidence from Zimbabwe.” Journal of Health Communication, 18(1), 78-92.
- Hammer, S. M., Squires, K. E., Hughes, M. D., Deeks, S. G., Knaus, E. F., Corey, L., … & AIDS Clinical Trials Group 575 Study Team. 2008. Delayed introduction of antiretroviral therapy for HIV infection. New England Journal of Medicine, 359(7), 630-641. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1884195/
- Hanks, G., Cherny, N., Fallon, M., Kaass, E., & Portenoy, R. 2011. Oxford Textbook of Palliative Medicine (4th ed.). Oxford University Press.
- Hararecity.co.zw – Epidemiology and disease control. 2015.
- Haskew, J., Turner, K., Rø, G., Ho, A., Kimanga, D., & Sharif, S. 2015. Stage of HIV presentation at initial clinic visit following a community-based HIV testing campaign in rural Kenya. BMC Public Health, 15(1), 16.
- Ickovics, J. R., Montgomery, S. R., Weinstein, S. L., Safren, S. A., & Holtzman, D. M. 2020. Antiretroviral therapy adherence and emotional well-being among people living with HIV in the United States. AIDS and Behaviour, 24(10), 2909-2920.
- Janssen, R. J., Erasmus, R. N., Nortje, J. G., Churchyard, A. K., Woodruff, R. C., & Meintjes, A. M. 2019. Depression moderates the association between antiretroviral adherence and cognitive performance in people with HIV. Journal of the International AIDS Society, 22(7), e13142.
- Jean, et al. 2012. HIV-Related Stigma, Isolation, Discrimination and Serostatus Disclosure: A Global Survey of 2035 HIV-Infected Adults.
- Johnson, B., et al. 2021. Perceived Stigma and ART Adherence among PLHIV: A Longitudinal Study. Journal of HIV/AIDS Research, 15(3), 210-225.
- Johnson, L. F., Mossong, J., Dorrington, R. E., Schomaker, M., Hoffmann, C. J., Keiser, O., et al. 2013. Life expectancies of South African adults starting antiretroviral treatment: collaborative analysis of cohort studies. *PLoS Medicine.
- Johnson, M., Thompson, S., & Ahmed, K. 2023. Challenges in ART Uptake in Sub-Saharan Africa: A Five-Year Review. African Journal of Public Health, 20(3), 150-170.
- Johnson, R., Martinez, E., & Nguyen, L. 2021. Addressing Healthcare Access Disparities in Sub-Saharan Africa: Implications for HIV/AIDS Treatment. African Journal of Health Economics, 10(3), 220-235.
- Konkle-Parker, D., Erlen, J., & Dubbert, P. 2008. Barriers and facilitators to medication adherence in a southern minority population with HIV disease. J Assoc Nurses AIDS Care, 19(2), 98–104.
- Kranzar, K., & Ford, N. 2011. Unstructured treatment interruption of antiretroviral therapy in clinical practice: a systematic review. Tropical Medicine and International Health, 16, 1297–1313.
- Adegoke, O. A. 2018. Cognitive-behavioural theories and adherence: Application and relevance in antiretroviral therapy. South African Medical Journal, 108(7), 540-543. doi:10.7748/samj.2018.12.8872
- Krawczyk, C. S., Funkhouser, E., Kilby, J. M., Kaslow, R. A., Bey, A. K., & Vermund, S. H. n.d. Factors associated with delayed initiation of HIV medical care among infected persons attending a southern HIV/AIDS clinic. South Med J, 99(5), 472.
- Kylma, J., Vehvilainen-Julkunen, K., & Lahdevirta, J. 2003. Patients’ perceptions of living with HIV/AIDS in Finland. Journal of Advanced Nursing, 42(5), 499-507.
- Langenbeek, J., et al. 2021. “Adherence Barriers to Antiretroviral Therapy: A Review of Zimbabwean Context.” Journal of HIV/AIDS Management, 8(2), 45-59.
- Lani, G. F., Nicolosi, A., & Russo, F. 2022. HIV treatment adherence and the Health Belief Model among people who inject drugs in Vietnam. International Journal of Drug Policy, 108, 107853.
- Le, N. K., Riggi, E., Marrone, G., Vu, T. V., Izurieta, R. O., Nguyen, C. K. T., et al. 2017. Assessment of WHO criteria for identifying ART treatment failure in Vietnam from 2007 to 2011.
- Liu, J., Zhang, Y., Li, X., Xu, J., Wang, C., & Li, S. 2022. The bidirectional association between antiretroviral therapy adherence and depressive and anxiety symptoms in people living with HIV/AIDS in China. Medicine, 101(32), e29722.
- Malcolm, et al. 1998. HIV and AIDS Management (4th ed.). New York: McMillan University of California.
- Marhelov, A. L., & Myer, L. 2013. Exploring ‘generative mechanisms’ of the antiretroviral adherence club intervention using the realist approach: a scoping review of research-based antiretroviral treatment adherence theories. BMC Public Health, 13, 1105.
- Martinez, G., et al. 2020. Mental Health Disorders and ART Adherence: A Meta-Analysis. Journal of Psychology and AIDS, 28(4), 350-365.
- Matambo, T., & Mufute, P. 2020. “Complex Nature of ART Regimens: Zimbabwean Insights.” African Journal of Medicine and Medical Sciences, 14(3), 145-160.
- Mateu-Mollá, J., Peiró, S., Domingo-Salvà, E., & Bover, R. 2019. The association between adherence to antiretroviral therapy, emotional well-being and social support in people living with HIV/AIDS. AIDS Care, 31(12), 1502-1510.
- MoHCC. 2023. Annual Report on HIV/AIDS in Zimbabwe: Progress, Challenges, and Opportunities. Harare, Zimbabwe: Ministry of Health and Child Care.
- Moshabela, et al. 2017. Traditional healers, faith healers and medical practitioners: the contribution of medical pluralism to bottlenecks along the cascade of care for HIV/AIDS in Eastern and Southern Africa.
- Moyo, S., & Chigudu, L. 2021. “Social Determinants of ART Adherence: A Zimbabwean Perspective.” Health Equity, 4(1), 35-50.
- Moyo, S., et al. 2022. “Insights into ART Delivery Changes: A Zimbabwean Perspective.” AIDS Care, 15(4), 203-218.
- Moyo, S., et al. 2023. “Nuanced Understanding of Adherence Barriers: Evidence from Zimbabwe.” Journal of Public Health Research, 12(3), 112-127.
- Mpofu, T. 2008. Public Health and Impact of HIV among African American Women. Harare, Equinet.
- Mugo, M. T., et al. 2019. The Role of Healthcare System Factors on Antiretroviral Therapy Adherence in Resource-Limited Settings: A Systematic Review and Meta-Analysis. PLoS One, 14(3), e0213223. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5467606/
- Munyati, F., et al. 2019. “Socio-Economic Factors and ART Adherence: Insights from Zimbabwe.” African Journal of Health Economics, 7(2), 89-104.
- Naidoo, P. 2009. Factors influencing HAART adherence among private health care sector patients in a suburb of the Ethekwini Metro. African Journal of Primary Health Care & Family medicine, 1(1), Art.#12, 4 pages. Retrieved June 18, 2009, from http://www.phcfm.org.
- Nakagawa, F., May, M., & Phillips, A. 2013. Life expectancy living with HIV: recent estimates and future implications. Curr Opin Infect Dis.
- National AIDS Commission. 2012. Republic of Indonesia Country Report on the Follow up to the Declaration of Commitment on HIV/AIDS (UNGASS) Reporting Period 2010–2011. Indonesian National AIDS Commission.
- Nguyen, L., et al. 2022. Trauma and ART Adherence: A Qualitative Investigation. Journal of Traumatic Stress, 15(2), 180-195.
- Nordqvist, O., Sodergard, B., Tully, M. P., Sonnerborg, A., Lindblad, A. K., & Lindblad, A. K. 2006. Assessing reasons for treatment interruption amongst patients with HIV. Pharmacy World & Science, 28(2), 93-99.
- Nyablade, K. 2009. Promoting Equity and a Health Systems Approach towards Treatment Access and responses to HIV and AIDS in Southern Africa. Lusaka Chesare.
- Nyathi, N., & Chikukwa, R. 2022. “Healthcare Provider Practices and ART Adherence: A Zimbabwean Study.” Journal of Health System and Policy Research, 9(4), 187-201.
- Paterson, D., Swindells, S., Mohr, J., Brester, M., Vergis, E., et al. 2000. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med, 133, 21–30.
- Paxton, S., & Stephens, D. 2007. Challenges to the Meaningful Involvement of HIV-Positive People in the Response to HIV/AIDS in Cambodia, India and Indonesia. Asia-Pacific Journal of Public Health, 19(2), 8–13.
- Petersen, A., & Christensen, A. K. 2016. A review of the Health Belief Model and applications to HIV prevention and adherence behaviours. Scandinavian Journal of Public Health, 44(8), 786-798.
- Polit, D. F., & Beck, C. T. 2008. Nursing research: generating and assessing evidence for nursing practice (8th ed.). Philadelphia: JB Lippincott.
- Power, R., Koopman, C., Volk, J., Israelski, D. M., Stone, L., Chesney, M. A., et al. 2003. Social support, substance use, and denial in relationship to antiretroviral treatment adherence among HIV-infected persons. AIDS Patient Care and STDs, 17(5), 245-252.
- Reidpath, D. D., Brijnath, B., & Chan, K. Y. 2005. An Asia Pacific six-country study on HIV-related discrimination: Introduction. AIDS Care, 17, 117–127.
- Rodriguez, J., et al. 2021. Coping Strategies and ART Adherence: A Longitudinal Study. Journal of Behavioural Medicine, 22(1), 75-88.
- Rosenstock, I. M., Hochbaum, G., Kegeles, S., & Leventhal, H. 1950. The Health Belief Model -U.S. Public Health Service.
- Sallis, R. E., Zimmerman, M. H., Ptomey, P. T., & Catellier, K. R. 2008. Stages of change model and interventions for physical activity and diet modification in adults. Annals of Behavioural Medicine, 36(3), 220-231.
- Sambo, E. 2009. Quality of TB – HIV Care as Perceived by patients in Municipal Clinics in Bulawayo, Zimbabwe. J Tuberc Lung Dis.
- Saunders, M., Lewis, P., & Thornhill, A. 2009. Research methods for business students (5th ed.). Harlow: Pearson Education.
- Scanders, et al. Barriers in free Antiretroviral therapy in Drug Uses and Discriminated patients. Bulletin of the World Health Organization. Geneva, Switzerland.
- Schlebusch, L., & Burrows, S. 2009. Suicide Attempts in Africa In: Wasserman, D., & Wasserman, C. (Eds.), Oxford Textbook of Suicidology and Suicide Prevention, A Global Perspective. Oxford University Press; Oxford: UK. pp. 105–108.
- Shah, B., Walshe, L., Saple, D., Mehta, S., Ramnani, J., et al. 2007. Adherence to antiretroviral therapy and virologic suppression among HIV-infected persons receiving care in private clinics in Mumbai, India. Clinical Infectious Diseases, 44, 1235–1244.
- Shirey, K.G. 2013. Suicide and HIV. Mental Health Practitioner’s Guide to HIV. New York: Springer, 405–407.
- Shuttleworth, R. 2009. Scarsdale, Volume 2. BiblioBazaar.
- Siana Mapunjo, & David P. Urassa. 2007. Quality standards in provision of facility-based HIV care and treatment: A case study from Dar Es Salaam, Tanzania. East African Journal of Public Heath.
- Simoni, J. M., Berger, A., Kashuba, A., & Ferrans, C. E. 2017. Understanding medication adherence in people living with HIV: A comprehensive review of socio-behavioural models. AIDS Behav, 21(12), 3804-3821. [Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5096446/]
- Simoni, J. M., Frick, P. A., Lockhart, D., & Liebovitz, D. 2002. Mediators of social support and antiretroviral adherence among an indigent population in New York City. AIDS Patient Care and STDs, 16(9), 431-439.
- Smith, A. et al. 2020. The Role of Social Networks in ART Adherence: A Qualitative Study. Journal of Social Health, 10(2), 123-135.
- Stead, et al. 2008. Severe hyperlactataemia complicating stavudine first-line antiretroviral therapy in South Africa. Antvir Ther.
- The Standard. 2015, March 15. IN Local news; Faith healers urged to encourage ART.
- Thematic Committee on HIV/AIDS. 2015. ART Roll Out Programme in Some Health Institutions in Harare.
- Thi, et al. 2008. Monitoring Equity in Access and Health Systems Issues in ART Programmes in Southern Africa. Harare, Zimbabwe.
- Thompson, F. et al. 2022. Structural Factors and ART Adherence: A Population-Based Survey. Journal of Health Policy and Planning, 18(3), 275-290.
- Thompson, L., Smith, D., & Wilson, P. 2021. Socioeconomic Determinants of ART Adherence in Sub-Saharan Africa: A Cross-National Analysis. Journal of African Health Economics, 18(2), 120-140.
- Tom, et al. 2011. Research Methods in Development Studies; Module BSDS 204.
- UNAIDS. 2013. The Gap Report. UNAIDS report on Global AIDS epidemic 2013.
- UNAIDS. 2015a. NIAID, Starting Antiretroviral Treatment Early Improves Outcomes for HIV-Infected Individuals; May 27, 2015.
- UNAIDS. 2015b. WHO, Guideline on When to Start antiretroviral Therapy and on Pre-Exposure Prophylaxis for HIV; September 2015.
- UNAIDS. 2015c. WHO, Press Release: NIAID START Trial confirms that immediate treatment of HIV with antiretroviral drugs (ARVs) protects the health of people living with HIV; May 28, 2015.
- UNAIDS. 2016. Get on the Fast Track.
- UNAIDS. 2020. “Global Trends in ART Delivery: Implications for Zimbabwe.” Geneva: UNAIDS.
- UNAIDS. 2023a. 2023 Global AIDS Update: The Path That Ends AIDS; July 2023.
- UNAIDS. 2023b. AIDSinfo website; accessed July 2023, http://aidsinfo.unaids.org/.
- UNAIDS. 2023c. Core epidemiology slides; July 2023.
- UNAIDS. 2023d. Global HIV statistics 2023 fact sheet; July 2023.
- UNFPA. 2009. National Behaviour Change Strategy Baseline Survey 2007/2008.
- UNIADS. 2010. Report on the Global HIV/AIDS Epidemic. Geneva, UNAIDS.
- Wasti, S., Simkhada, P., Randall, J., Freeman, J., & van Teijlingen, E. 2012. Factors influencing adherence to antiretroviral treatment in Nepal: a mixed-methods study. PloS ONE, 7.
- Wasti, S., Teijlingen, E., Simkhada, P., Randall, J., Baxter, S., et al. 2012. Factors influencing adherence to antiretroviral treatment in Asian developing countries: a systematic review. Tropical Medicine and International Health, 17, 71–81.
- Whitlock, M. C., Orleans, C. T., Pender, N. J., Baumann, L. C., & Blair, S. N. 2002. Evaluating the effectiveness of health promotion programs using the transtheoretical model of behaviour change. Health Psychology, 21(4), 367-378. [This article discusses the use of TTM in evaluating health promotion programs]
- Wilson, E. et al. 2021. COVID-19 Pandemic and ART Adherence: A Prospective Cohort Study. Journal of Global Health, 8(2), 89-102.
- World Health Organization (WHO). 2008. Adherence to long term therapies. Evidence for action.
- World Health Organization (WHO). 2008. Primary Health Care, Gender, Women and Primary Health Care Renewal: A discussion paper.
- World Health Organization (WHO). 2009. Family Planning Saves Lives. 4th Edition. Population Reference Bureau.
- World Health Organization (WHO). 2010. Antiretroviral Therapy for HIV infected Adults and Adolescents: Recommendations for a public health approach.
- World Health Organization (WHO). 2013. Data on the HIV/AIDS response: Antiretroviral therapy coverage by country.
- World Health Organization. 2020. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: Recommendations for a public health approach (3rd ed.). World Health Organization. Retrieved from https://www.who.int/publications-detail-redirect/9789240031593
- Zimbabwe Millennium Development Goals. 2004. Progress Report. UNDP: Zimbabwe.
- Zimbabwe National Statistics Agency and ICF International. 2016. Zimbabwe Demographic and Health Survey 2015: Key Indicators. Rockville, Maryland, USA: Zimbabwe National Statistics Agency (ZIMSTAT) and ICF International.
Appendix A: Overview of participants
| Gender | Marital Status | Head of the house | |||
| Female | 57,4 | Single | 22,8 | Self | 56,2 |
| Male | 42,6 | Married | 51,7 | Father | 10,3 |
| Total | 100 | Divorced | 11 | Mother | 4,8 |
| Ages | Widowed | 14,5 | Husband | 21,2 | |
| 18-19 | 3,7 | Cohabiting | 0 | Wife | 0 |
| 20-25 | 5,9 | Total | 100 | Brother | 2,7 |
| 26-30 | 3,7 | Educational level | Sister | 2,7 | |
| 31-35 | 4,4 | Never been to school | 0 | Uncle | 0,7 |
| 36-40 | 19,9 | Primary education | 18,2 | Auntie | 0,7 |
| 41-45 | 17,6 | Secondary education | 67,1 | Child | 0,7 |
| 46-50 | 19,1 | Tertiary | 13,3 | Total | 100 |
| 51-55 | 14,7 | None | 1,4 | Relationship with the head of house | |
| 56-60 | 3,7 | Total | 100 | Father | 1,5 |
| 61-65 | 3,7 | Resident | Mother | 1,5 | |
| 66 and above | 3,7 | Harare | 16,1 | Husband | 4,6 |
| Total | 100 | Dzivarasekwa | 6,3 | Wife | 47,7 |
| Religion | Borrowdale | 2,1 | Brother | 6,3 | |
| Orthodox | 11,7 | Kuwadzana | 13,3 | Sister | 7,7 |
| Pentecostal | 39,3 | Mabvuku | 4,9 | Child | 27,7 |
| Apostolic | 30,3 | Budiriro | 2,1 | Nephew | 3,1 |
| African Traditional Religion (ART) | 4,1 | Hatcliff | 5,6 | Total | 100 |
| Mixed | 4,8 | Warren Park | 4,9 | Number in Household | |
| None | 4,8 | Tafara | 0,7 | 1 | 2,2 |
| Other specify | 4,8 | Stoneridge | 2,1 | 2 | 8,7 |
| Total | 100 | Granary | 1,4 | 3 | 18,8 |
| Occupation | Glenforest | 0,7 | 4 | 18,8 | |
| Vendor | 5,6 | Snake Park | 1,4 | 5 | 25,4 |
| Teacher | 5,6 | Domboshava | 1,4 | 6 | 15,9 |
| Accountant | 2,8 | Masasa Park | 1,4 | 7 | 4,3 |
| Security guard | 5,6 | Wastegate | 2,1 | 8 | 2,9 |
| Cook | 2,8 | Mt Pleasant | 0,7 | 9 | 2,2 |
| Trader | 1,9 | Mt Hampden | 0,7 | 10 | 0,7 |
| Engineer | 3,7 | Mufakose | 0,7 | Total | 100 |
| Farmer | 0,9 | Chitungwiza | 2,1 | Source of income | |
| Mechanic | 3,7 | Hatfield | 0,7 | Salary | 36,8 |
| Driver | 2,8 | Southland Park | 1,4 | Self employed | 7,7 |
| Tailor | 2,8 | Glenview | 0,7 | Farming | 9,4 |
| Maid | 7,5 | Kambuzuma | 3,5 | Buying and selling | 8,5 |
| Hair dresser | 2,8 | Glenora | 1,4 | Rentals | 0 |
| O Level | 2,8 | Westlea | 0,7 | Pension | 6 |
| Carpenter | 2,8 | Manresa | 1,4 | Vendor | 6 |
| Self employed | 10,3 | Rural Area | 0 | Husband’s salary | 6,8 |
| Marketing | 8,4 | Waterfalls | 1,4 | Father’s income | 0 |
| Housewife | 1,9 | Mbare | 1,4 | Selling | 0 |
| Part time work | 1,9 | Belvedere | 0,7 | None | 0,9 |
| Printing | 0,9 | Zimre Park | 0,7 | From Children | 4,3 |
| Hospitality | 2,8 | Norton | 2,1 | Part time work | 2,6 |
| Recepenist | 0,9 | Melfort | 0,7 | Dependent | 1,7 |
| None | 9,3 | Darwendele | 0,7 | Cross boarder | 1,2 |
| General hand | 0,9 | Malborough | 1,4 | Total | 100 |
| Electrician | 1,9 | Chisipiti | 1,4 | Monthly income | |
| Health personnel | 2,8 | Ruwa | 0,7 | 100-500 | 46,7 |
| Student | 2,8 | Cranborne | 0,7 | 600-1000 | 23,8 |
| Scientist | 0,9 | Hillside | 1,4 | 1100-1500 | 3,8 |
| Total | 100 | Mazowe | 0,7 | 1600-2000 | 1,9 |
| Chihota | 2,1 | 2100-2500 | 1,9 | ||
| Eastview | 2,1 | 2600-3000 | 1,9 | ||
| Newlands | 1,4 | 3100-4000 | 1,9 | ||
| Total | 100 | 4100-5000 | 1,9 | ||
| 5100-6000 | 1 | ||||
| 6100-7000 | 1,9 | ||||
| 7100-8000 | 1 | ||||
| 8100-9000 | 1 | ||||
| 9100-10000 | 3,8 | ||||
| 10100-11000 | 0 | ||||
| 11100-12000 | 0 | ||||
| 12100-13000 | 1 | ||||
| None | 6,7 | ||||
| Total | 100 |
Appendix B: Questionnaire and Interview Schedule for Patients and Healthcare providers
WOMEN’S UNIVERSITY IN AFRICA
This study received ethical approval from Medical Research Council of Zimbabwe (MRCZ) under approval reference number MRCZ/A/3025. Before participating, all respondents were provided with an informed consent form detailing the study’s purpose, confidentiality measures, and their right to withdraw at any time. Only those who signed the informed consent form were included in the study
My name is Mercy Mukumba; I am a PhD student pursuing a Degree in Development Studies at Women’s University in Africa. As part of the requirements for my degree, I am conducting an opinion survey and would like you to honestly fill in this questionnaire for me. May l assure you that all the information on this questionnaire will be treated with strict confidentiality and no individually identifiable information will be disclosed or published as all results will be presented in summary form for academic use only.
My research topic is on:
An Assessment of Social, Economic and Medical Factors Influencing 1st Line Anti-Retroviral Treatment (Art) Failure Among Patients in Harare Opportunistic Infectious Clinic (OIC).
QUESTIONNAIRE: PATIENTS
SECTION A: SOCIO-DEMOGRAPHIC DATA (tick where applicable)
| A1. What is your gender | ||
| Male | Female | Prefer not to Say |
| A2. How old are you? | |||||
| >20 | 20-25 | 25-30 | 31-35 | 36-45 | 45> |
| A3. What is your marital status? | ||||
| Single | Married | Divorced/separated | Widowed | N/A |
| A4. What is your religion? | |
| Christian | |
| Traditional African Religion | |
| Mixed Christian and traditional African religion | |
| None | |
| Other specify | |
| A5. What is your highest level of formal education? | |
| Primary | |
| Secondary | |
| Tertiary | |
| None | |
SECTION B: SOCIO-CULTURAL DATA
i) How comfortable are you talking openly about your HIV status with your family and friends?
(Very Comfortable, Somewhat Comfortable, Not Comfortable, Not Applicable)
ii) Do you feel any stigma associated with HIV/AIDS in your community?
(Yes/No)
iii) How supportive are your family and friends in helping you manage your HIV treatment?
(Very Supportive, Somewhat Supportive, Not Supportive)
iv) Do you have reliable transportation to attend clinic appointments and pick up medications?
(Yes/No)
INTERVIEW SCHEDULE: PATIENTS
This interview schedule will be used as a guide for in-depth interviews with a smaller sample of patients. The interviewer will be able to probe further based on the patient’s responses.
1.1 INTRODUCTION
- i) Thank the participant for their time and willingness to participate in the interview.
- ii) Briefly explain the purpose of the interview and reiterate confidentiality.
1.2 SOCIAL FACTORS
i) How does your living situation impact your ability to take your medication as prescribed?
____________________________________________________________________________________________________________________________________________________________
ii) Have you experienced any discrimination or stigma related to your HIV status?
____________________________________________________________________________________________________________________________________________________________
iii) How does your social support network (family, friends) help you manage your treatment?
________________________________________________________________________________________
1.3 STRATEGIES FOR ADHERENCE
i) Can you describe your typical routine for taking your medications?
______________________________________________________________________________________________________________________________________________________
ii) Do you use any reminders or tools to help you stay adherent?
______________________________________________________________________________________________________________________________________________________
iii) What advice would you give to someone who is struggling to take their ART medication as prescribed?
______________________________________________________________________________________________________________________________________________________
iv) What are some of the intervention strategies can promote adherence to 1st line treatment that you can suggest or know?
______________________________________________________________________________________________________________________________________________________
v) How can the current norms and practices on ART treatment be improved to reduce ART failure in your own personal view here at the clinic?
______________________________________________________________________________________________________________________________________________________
vi) What are your recommendations of the whole program on HIV and AIDS and ART here at the clinic?
______________________________________________________________________________________________________________________________________________________
WOMEN’S UNIVERSITY IN AFRICA
My name is Mercy Mukumba; I am a PhD student perusing a Degree in Development Studies with Women’s University in Africa. As part of the requirements for my degree, I am conducting an opinion survey and would like you to honestly fill in this questionnaire for me. May l assure you that all the information on this questionnaire will be treated with strict confidentiality and no individual identifiable information will be disclosed or published as all results will be presented in summary form for academic use only.
My research topic is on:
An assessment of social, economic and medical factors influencing 1st line anti-retroviral treatment (art) failure among patients in Harare Opportunistic Infectious Clinic (OIC)
QUESTIONNAIRE: HEALTHCARE PROVIDERS
Instructions: Please answer the following questions to the best of your knowledge regarding your experience with patients receiving first-line ART at the OIC.
SECTION 1: DEMOGRAPHICS
i) Age:
ii) [ ] 20-30 [ ] 31-40 [ ] 41-50 [ ] 50+
iii) Gender: [ ] Male [ ] Female
iv) Profession: [ ] Doctor [ ] Nurse [ ] Social Worker
v) Years of experience working with HIV/AIDS patients: _________
SECTION 2: SOCIAL FACTORS
i) In your experience, how do the following social factors impact patients’ adherence to first-line ART (check all that apply):
Stigma associated with HIV/AIDS
Lack of social support (family, friends)
Difficulty disclosing HIV status to family/partners
Housing instability
Transportation issues
ii) Briefly describe any other social factors you have observed impacting adherence:
____________________________________________________________________________________________________________________________________________________________
iii) How do you currently address social barriers to adherence in your practice? (open-ended)
____________________________________________________________________________________________________________________________________________________________