
The influence of Vitamin B12 on the Progression of Fracture Healing in Rats.
- Mana, H. P.
- Mutah, A. A.
- Mohzo, D. L.
- Hermon, W.
- 382-391
- Jul 12, 2024
- Health And Cybersecurity
The Influence of Vitamin B12 on The Progression of Fracture Healing in Rats.
1*Mana, H. P., 2,4 Mutah, A. A., 3Mohzo, D. L., 2Hermon, W.
1Veteriary Teaching Hospital, University of Maiduguri, PMB 1069, University of Maiduguri, Nigeria;
2Department of Veterinary Surgery and Radiology, Faculty of Veterinary Medicine, PMB 1069, University of Maiduguri, Nigeria;
3Department of Veterinary Pathology, Faculty of Veterinary Medicine, PMB 1069, University of Maiduguri, Nigeria.
4Bioengineering Department, Sinclair Lab, 7 Asa Drive, Suite 205 Bethlehem, PA 18015 USA.
DOI: https://doi.org/10.51244/IJRSI.2024.1106030
Received: 14 May 2024; Revised: 04 June 2024; Accepted: 11 June 2024; Published: 12 July 2024
ABSTRACT
Bone fracture is a complete or partial breakage of the bone structure. Bone fracture occurs when the bone structure is either completely or partially broken. The process of healing involves the regeneration of new bone tissue, which seamlessly integrates with the uninjured bone. Fracture repair entails rejoining and realigning the broken bone ends to facilitate healing. Previous reparative studies to enhance repair were limited in incorporating a therapeutically active factor to facilitate repair. Cyanocobalamin, a synthetic form of vitamin B12, is readily converted in the body into its active forms, methylcobalamin and cobamamide. In this study, 30 rats were obtained from a reputable breeder (University of Maiduguri staff quarters, line F house No. 1), acclimatized for 21 days, and divided into two groups: Group A, receiving vitamin B12 (15 rats), and Group B, serving as the control (15 rats) recived placebo (normal saline). Group A received a dosage of vitamin B12 at 500 micrograms/kg, while Group B remained untreated. Samples from fractured tibiae were collected at two weeks intervals on days 14, 28, and 42, respectively. These samples were decalcified using formic acid, stained with Hematoxylin and Eosin (H&E), and examined under a microscope at magnifications of X10, X40, and X100. We used qualitative data analysis method to analyse our results. However, based on qualitative analysis, there were noticeable gross and histological disparities on days 28 and 42. These findings suggest that vitamin B12 supplementation enhances collagen formation on days 28 and 42, potentially improving fracture repair using the qualitative data analysis method.
Keywords: Fracture, Rats, Vitamin B12, Histology, Collagen
INTRODUCTION
Successful primary bone healing hinges on firm stabilization, with or without compression at the bone ends. This stability inhibits callus formation in both cancellous and cortical bone, as noted by Ghiasi et al., 2017). Moreover, primary bone healing encompasses two distinct processes: gap healing and contact healing. Both methods facilitate bone union without forming external callus or any fibrous tissue or cartilage within the fracture site (Vharles, 2007). Fracture repair relies on the precise expression of numerous genes, each activated and deactivated at specific stages of the healing process. Key genes involved include transforming growth factors (TGF), fibroblast growth factor (FGF), platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), bone morphogenetic proteins (BMP), osteonectin, osteocalcin, osteopontin, fibronectin, bone morphogenetic protein receptor (BMPR), Smads, interleukins (IL-1, IL-6), granulocyte-macrophage colony-stimulating factor (GM-CSF), and macrophage colony-stimulating factor (M-CSF). The regulation of these genes facilitates cellular interactions, thereby promoting the restoration of bone structure and function. The four-stage model originated as the result of histological observations of healing fractures in both human patients and animal models. However, the past several decades’ research has explored the cellular and molecular forces that drive the underlying processes (Al-Aql et al., 2008). At the cellular level, inflammatory cells, vascular cells, osteochondral progenitors, and osteoclasts are key players in the repair process. At the molecular level, fracture repair is driven by the three main classes of factors: pro-inflammatory cytokines and growth factors, pro-osteogenic factors, and angiogenic factors (Barnes et al., 1999). These help establish the relevant morphogenetic fields by recruiting cells and stimulating growth and/or differentiation.
Thereafter, the damaged soft tissues are repaired and the fracture is covered by soft callus and later hard callus. The bridging hard callus is eventually remodeled to re-establish the original geometry and function of the damaged tissue. In certain circumstances where there is absolute stability, or in well-apposed metaphyseal fractures, and even without the appearance of an intermediate cartilaginous soft callus, intramembranous hard callus formation may dominate (Schindeler et al., 2008). A lot of fractures have some degree of mechanical instability and heal by endochondral ossification bony callus formation is preceded by a cartilaginous template (Gerstenfeld et al., 2003). This stage is dominated on a cellular level by chondrocytes and fibroblasts, although the relative proportions of the different cell types can vary between fractures. These cells produce a semi-rigid soft callus that is able to provide mechanical support to the fracture, as well as act as a template for the bony callus that will later supersede it. Cartilaginous callus is principally avascular, although its subsequent replacement with woven bone involves vascular invasion.
Chondrocytes derived from mesenchymal progenitors proliferate and synthesize cartilaginous matrix until all the fibrinous/granulation tissue is replaced by cartilage. Where cartilage production is deficient, fibroblasts replace the region with generalized fibrous tissue (Mutah et al., 2023). Discrete cartilaginous regions progressively grow and merge to produce a central fibrocartilaginous plug between the fractured fragments that splints the fracture (Barnes et al., 1999). In the final stages of soft callus production, the chondrocytes undergo hypertrophy and mineralize the cartilaginous matrix before undergoing apoptosis.
Fibroblast proliferation and chondrocyte proliferation/differentiation are stimulated by the coordinated expression of growth factors including TGF-2 and -3, PDGF, fibroblast growth factor -1 (FGF-1), and insulin-like growth factor (IGF) (Narine et al., 2006). Additionally, members of the BMP family (BMP -2, -4, -5 and -6) assist in promoting cell proliferation and chondrogenesis. In response to these factors, chondrocytes are able to generate considerable amounts of extracellular matrix proteins, particularly collagen II (or collagen X for hypertrophic chondrocytes) (AI-Aql et al., 2008). Invasion of the soft callus by vascular endothelial cells, angiogenesis, and capillary in-growth is stimulated by pro-angiogenic factors including VEGF, BMPs, FGF-1 and TGF (Beamer et al 2010). VEGF expression by osteogenic cells is dependent on the master bone and cartilage regulatory factor Cbfa1/ Runx2 (Kwon et al., 2011), and is not highly expressed by the early mesenchymal/inflammatory tissue at the fracture site (Pufe et al., 2002). In addition, angiopoietin I and II regulate vascular morphogenesis of larger vessels and development of collateral branches from existent vessels (AI-Aql et al., 2008). Also known as primary bone formation (Gerstenfeld et al., 2003), this stage represents most active period of osteogenesis. It is characterized by high levels of osteoblast activity and the formation of mineralized bone matrix, which arises directly in the peripheral callus in areas of stability.
In order for bridging new hard callus to form, the insecure soft callus is gradually removed, concomitant with revascularization (Mana et al., 2023). The new bone is known as the hard callus and it is typically irregular and under-remodeled. Notably, hard callus can form in the absence of a cartilaginous template in intramembranous bone formation (during conditions of high mechanical stability) or in appositional bone growth, where bone forms directly adjacent to an existing mineralized surface (Mana et al., 2023). Nevertheless, in most orthopedic cases, such as fractures involving long bones such as the radius and ulna, tibia and fibula, or femoral fractures, there exists some degree of endochondral ossification (Mana et al., 2022).
The primary composition of woven bone comprises a combination of protein-based and mineralized extracellular matrix tissue. This matrix is synthesized by mature osteoblasts, which arise from osteoprogenitor cells and are influenced by osteogenic factors (Mana et al., 2023). Members of the BMP family are critical mediators of this process, and have been shown to be sufficient for de novo bone formation (Chen et al., 2004). Other growth factors are expressed during this time, although it is unclear whether their impact on bone healing predominantly affects osteoprogenitor migration/proliferation versus osteogenic differentiation (Gerstenfeld et al., 2003). The source(s) of osteoprogenitor responsible for fracture healing is yet to be understood clearly. The periosteum is a rich source of stem cells able to produce bone and bone healing is often delayed when the periosteum is damaged or stripped (Colnot, 2009). The bone marrow also contains mesenchymal stem cells capable of contributing to bone formation during repair (Lin et al., 2019). However, bones are able to mount an effort at healing, including hard callus formation, even in the absence of periosteal and/or marrow osteoprogenitors. Thus it is possible that osteoprogenitors may originate from multiple sources including the circulation the vasculature and surrounding local tissues (Lin et al., 2019). The vasculature is known to be critical for formation of the hard callus, with increased oxygen tension in the local region necessary for osteoblast differentiation. Stimulation of vessel formation using angiogenic factors can augment bone formation and fracture healing in model systems (Hankenson et al., 2011). However, recent studies have shown that delayed union can occur even after the vasculature has been re-established, indicating that the blood supply alone is not the only determinant of fracture healing success (Tarantino et al., 2009). Vitamin B12 is a cobalt-containing B complex vitamin needed for the formation of red blood cells, for normal nerve cell activity and for the synthesis of DNA during cell division.(Halczuk et al., 2023). Cyanocobalamin is a synthetic form of vitamin B12 that is easily converted in the body to its bioactive forms, methylcobalamin and cobamamide (Alejandro et al., 2005). The mechanism of action of this vitamin in the microarchitecture of bones is not yet well clear, but some studies suggested that it either modulate the formation of collagen or alter the metabolism of osteoblasts, always in a dose-dependent manner (Barley et al., 2017). Low levels of vitamin B12 can predispose to low bone mineral density and increased risks of fractures in individuals (Ebesunun et al., 2014) (Clarke et al., 2015). However, the results are not yet conclusive and the actual impact of vitamin B12 deficiency on bone health and the mechanisms associated with bone metabolism is not well established (Macedo et al., 1992).
MATERIALS AND METHOD
Experimental Animals Thirty rats of both sexes, aged 8 weeks, weighed 800 ± 10 grams were utilized for this study. They were procured locally from the University of Maiduguri quarters, Line F, House No. 1, Maiduguri, Borno state. The rats underwent a 3-week acclimatization period in a designated section of the wet lab of Veterinary Surgery and Radiology. They were then divided into two groups (A and B), each comprising 15 rats. The housing consisted of two black rubber containers covered with mesh wire, with sawdust as bedding. The rats had access to poultry feed (Ultimum feed and Breedwell broiler finisher) and water ad libitum. The bedding was changed every 3 days. The research was conducted during the months of September, October, and November 2021, under ambient temperature conditions.
a). Ethical clearance
Approval for the Animal Utilization Protocol was secured from the Faculty of Veterinary Medicine, University of Maiduguri, on February 1, 2023, with reference number FVM/UNIMAID/AUEC/2022/001. The approved timeframe extends from February 1, 2023, to July 30, 2023. Therefore, we utilized the granted permission within the specified period.
b). Surgical Procedure
Each rat’s weight was measured using a digital sensitive scale and recorded. Anesthesia was induced using 1ml of 100% halothane soaked in 2g of cotton roll. The right and left tibia and fibula of rats weighing between 0.4-0.5kg were fractured using a fracture device based on the 3-point bending principles. An improvised intramedullary pin (23 Gauge needle) was inserted proximally through the articular surface of the medial condyle and driven into the medullary canal up to the distal part of the tibia to achieve closed reduction. The protruding part of the pin was then cut at the cortical level of the bone. Treatment Regimen Group A (15 rats) received intramuscular injections of 1ml of inj. cyanocobalamin 500 microgram (Hangzhou Norobio pharmaceutical co. ltd. Hangzhou, China) on daily basi. Group B (15 rats) served as the control group and received 1 ml of placebo (Normal Saline) daily. Samples were collected from both groups at day 14, 28, and 42 after euthanizing the animals with overdosed halothane. The samples were preserved in 10% formalin in sample bottles and submitted to University of Maiduguri Teaching Hospital’s histopathology laboratory for processing.
c). Decalcification of fracture limb
The tibia of all experimental animals was harvested and fixed in 5% formaldehyde for 24 hours. Samples were then washed under tap running water and placed in decalcifying solution containing formic acid. The decalcifying solutions were changed daily for 3 days until the bone was easily penetrated by a needle without force. Heavy-duty microtomes were used to section the bone tissues.
d). Histopathology
Hematoxylin and eosin (H&E) staining was conducted following routine protocols. Transverse sections of 5 micrometer were stained with hematoxylin solution for 5 min followed by 5 dips in 1% acid ethanol and rinsed in distilled water. Subsequently, sections were stained with eosin solution for 3 min, dehydrated with graded alcohol, cleared with xylene, and mounted slides were examined and photographed using an Omax microscope (USA).
e). Anaesthesia
During the anaesthetic induction using 1ml of Halothane on a cotton wool ball, all rats defecated. It took 2-3 minutes for complete anaesthesia, with varying onset times; some rats showed immediate sedation within seconds, while others required longer. For rats not fully anaesthetized, an additional 0.5 ml of Halothane was added. Initially, rats reacted by attempting to escape the chamber, followed by slowed movement and eventual rest in a sedated state with a bent back. They eventually became recumbent in lateral, dorsal, or sternal positions, indicating loss of sensation and consciousness. Rats regained consciousness approximately 2-3 minutes after anaesthesia.
Immediately the rats were fully anesthetized, an intramedullary pin was inserted, and a transverse fracture was induced at the mid-shaft of the tibia. Upon recovery from anesthesia, 80% of the rats demonstrated the ability to bear weight on and use the fractured limb with a normal gait, exhibiting no reduction in movement or activity. However, 20% displayed signs of limping, with some dragging the limb until the following day before returning to their normal gait.
f). Post operative care
No post-operative complications were observed among the rats. They all began bearing weight on the affected limb immediately after surgery, indicating effective fracture immobilization. No analgesics or antibiotics were administered in this study due to the absence of open wounds. Additionally, we refrained from using analgesics and antibiotics to prevent any potential interference with our experimental outcomes.
RESULTS
Moreover, on postoperative day 14, the cellular composition of the fracture exhibited sparsely distributed collagen, with distinct fibroblasts (black arrow), prominent osteoblasts (blue arrow), and few chondrocytes (pink arrow), along with marked cellular infiltration (Figure 1A). In Figure 1B, moderate collagen formation was observed, accompanied by the presence of mononuclear cells (black arrow) and chondrocyte formation (blue arrow) at the periphery. Additionally, the presence of debris and hematoma formation around the fracture site was noted in both groups of rats on day 14 of the study (Figure 1). This suggests that tibial osteotomy resulted in injury, causing disruption of blood vessels and subsequent hematoma and debris accumulation at the fracture site. There were no significant differences observed in the histological sections between the Vitamin B12-treated and control groups on day 14.
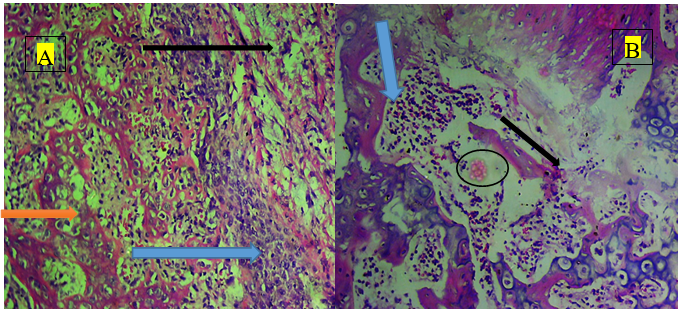
Day 14
Figure 1A; B12-treated group: The fracture zone exhibited sparse collagen distribution with distinct fibroblasts (black arrow), prominent osteoblasts (blue arrow), and few chondrocytes (pink arrow), accompanied by marked cellular infiltration.
B; Control Group: sparse collagen formation was observed, along with the presence of mononuclear cells (black arrow) and chondrocyte formation (blue arrow) at the periphery and the presence of hematoma black circle.
In this study, fracture repair progressed through the process of endochondral ossification. Histological examination revealed cellular changes corresponding to various stages of inflammation, soft and hard callus formation, and remodeling, depending on the phase of the fracture process. Upon euthanasia and tibial dissection, the gross appearance of the fracture indicated evident callus formation on the right tibia and it is characterized by elevated perimeter contour around the fractured ends (black circle) compared to the left tibia (Figure 2), which is more in the Vitamin B12 treated group as when compared with the control group (Blue Circle)
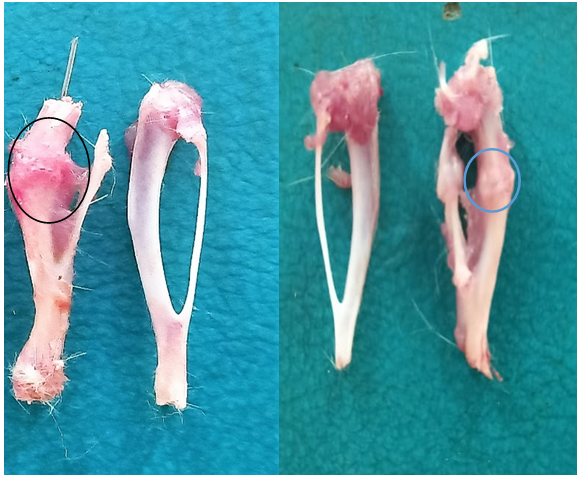
Figure 2: Day 28; Gross findings
Figure 1: A; The Vitamin B12 group exhibited a larger elevation in callus perimeter contour around the fractured end.
B; The control group showed a moderate elevation in callus perimeter contour around the fractured end.
Furthermore, histologically, on day 28 of the Vitamin B12-treated group, a fracture zone was observed, characterized by numerous vascular channels (black arrows), along with numerous chondrocytes exhibiting marked collagen deposition. Additionally, there was an increase in cancellous bone, accompanied by the appearance of hypertrophic chondrocytes, bone marrow, and osteoid callus formation. The hard callus volume was notably significant and hypercellular, displaying bone matrix formation and an admixture of loose connective tissue and osteoclasts (Figure 3A). This substantial hard callus volume is believed to provide additional strength to the fracture site, thereby preventing excessive movement and potential recurrence of fracture. However, in the control group, numerous mononuclear cells (black arrow) were observed, along with collagen deposition and the presence of osteocytes.
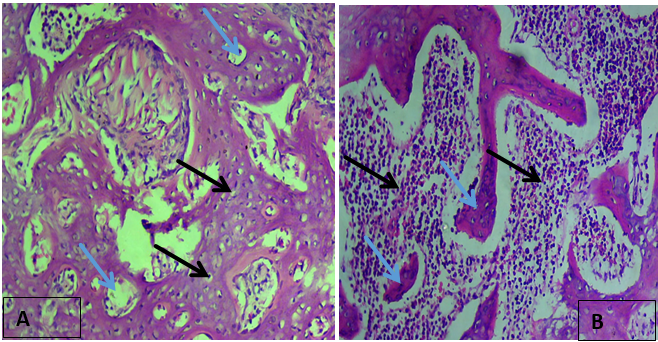
Figure 3 Day 28; Histological findings
Figure 3: A; B12 Treated group: Zone of fracture typified by numerous vascular channels (blue arrows), numerous chondrocytes with marked collagen deposition (Black arrow).
B; Control group: Numerous mononuclear cellular infilteration (black arrow) with Scanty collagen deposition (blue arrow).
By day 42, the rats treated with Vitamin B12 displayed significant mineralization and lamellar bone formation. This pronounced mineralization indicated complete union, characterized by bone matrix proliferation, heightened mineralization, and medullary recanalization. Moreover, there was evidence of medullary cavity formation along with increased cartilage matrix hypercellularity. Additionally, the formation of Howship lacunae and periosteum was noted in the treated group, indicating late stage of remodelling. However, in the control group, we observed scanty lamella bones, remnants of collagen (Scanty) with numerous osteocytes, marked Howship lacunae (red arrow) and presence of few fibroblasts signifying early remodelling stage. Graphical representation shows that there difference between the treated group and our control as seen below.
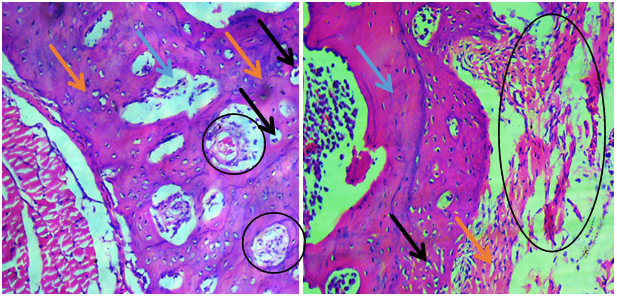
Figure 4; Day 42 histological findings
A: Vitamin B12 treated group.
Zone of fracture showing marked osteoclastic activity with prominent Howship lacunae (blue arrow), predominant lamella bone (pink arrow), fibroblast and osteoblast present on the periosteum (Black arrow) and haversian canal formation (black circle).
B: Control group: Zone of fracture typified by presence of lamellar bone (blue arrow) with numerous osteocytes, scanty collagen deposition (black circle) and presence of few fibroblasts (pink arrow).
Therefore, the Slides obtained from each group for days 14, 28 and 42 were scored individually using a suitable fracture scoring pattern. We followed the fracture healing pattern of Sağliyan et al., 2016. An average score was taken for each group. Descriptive statistics was used to analysed the effect of vitamin B12 on fracture repair progression and was represented graphically.
Table 1. The scoring system used to assess histological healing of fractures adopted from Sağliyan et al., 2016.
| Score | Tissues Present |
| 1 | Empty Cavity |
| 2 | Fibrous tissues only |
| 3 | More fibrocartilage than Fibrous tissues |
| 4 | Fibrocartilage only |
| 5 | More Fibrocartilage than Bone |
| 6 | More Bone than Fibrocartilage |
| 7 | Bone Only |
Table 2. Fracture healing score of Vitamin B12 treated group and control
| Days | Vit. B12 treated | Control |
| 14 | 1.0 | 1.0 |
| 28 | 3.0 | 2.0 |
| 42 | 7.0 | 5.0 |
Figure 5: Bar chart Comparing Vitamin B12 and Control group.
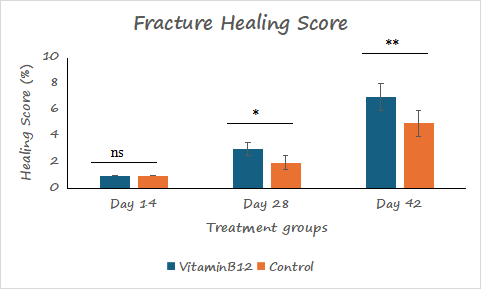
Figure 5. A bar chart of fracture healing score. No observable difference was noticed between the Vit B12 treated group compared to the control at day 14; however, a significant difference was observed on days 28 and 42 post-therapy with Vit B12 compared to the control.
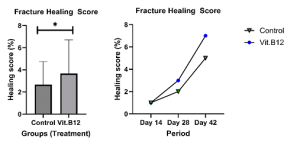
Figure 6 A and B: Showing a clear graphical representation of the Vitamin B12 treated group and the control group using bar chat and graph plot.
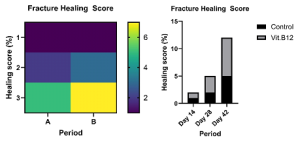
Figure 7 A and B: Graphical representation of both the treated and control group
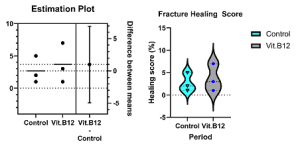
Figure 8 A and B: indicating estimation plot expressing the difference between the means of the healing score of both the treated and control group.
DISCUSSION
Fracture creation in this research resulted in minimal soft tissue reaction, and absence of bone comminution, hence, the skin remained intact. Closed reduction of fracture is now the most suitable model used to appraise fracture repair process, since the periosteum and the soft tissue surrounding the fracture site play a vital role during fracture repair process (Handool et al., 2018). Techniques such as osteotomy, bone drills and use of blunt guillotine-like apparatus to induce fracture are characterized by undesirable effects and recurrent complications including death, misplaced fracture, excess comminution and deep infection (Aurégan et al., 2013; Haffner-Luntzer et al., 2016). Comminutions arising from fractured bone varies in different degrees hence making it difficult to control during fracture healing (Pei and Fu, 2011; Ghiasi et al., 2017). As the degree of fracture comminution can affect the formation of callus, there was association between the rat fracture model used with the resultant comminution and the soft callus produced. Manually inflicted fractures with either internal or external fixation have been described by several authors as a model to study fracture healing. The inadequate stability of internal or external fixation leads to variable degrees of displacement and repeated movement of the bone fragments during the healing period (Glatt et al.,2017). The guillotine-like apparatus technique bone fractures in rat tibiae showed minor comminution but high displacement of bone fragment, bending and pin angulation of more than 10° (Aurégan et al., 2013). Additionally, the rat model of femoral fracture had an IM pin inserted through the knee in a retrograde fashion to induce osteosynthesis; then a fixed weight dropped onto the bone placed on a blunt guillotine to create a standardized closed mid-shaft fracture of the rat femur (Aurégan et al., 2013). The fractures created resulted death, deep infection, non-acceptable fracture or comminution. Hulth (1989) used manual force to produce a closed fracture model of the rat tibia but it was difficult to control or reproduce in a standard manner, making the method unsuitable as a model. Recent findings indicate that the exact effect of vitamin B12 deficiency in bone health, bone fracture and the mechanisms associated with bone metabolism is not well established (Macêdo et al., 2017). In this study, we did not noticed any qualitative difference between the Vitamins B12 treated group and the control group on day 14. Vitamin B12 may not have any observable effect when administered simultaneously for 2 weeks post fracture. However on day 28, we noticed some qualitative changes on the Vitamin B12 group, having dense collagen deposition as compared with control as presented graphically using Bar Chart. However, this study contradicts the findings of Holstein et al. (2010), who claimed that Vitamin B12 and folate deficiency does not impact fracture repair in rats. Conversely, our results align with those of Barley et al. (2017), who proposed vitamin B12 augmentation may either modulate collagen formation or alter osteoblast metabolism, consistently showing dose-dependent effects. Furthermore, on day 42, the few woven bone with marked lamella bone formation in the Vitamin B12 treated group suggest a faster healing rate as compared to our control group which has more woven bone and less lamella bone, as shown by bar chart representation. Therefore, this research shows that vitamin B12 given for an extended period of time improves collagen deposition and may even promote the formation of lamellar bone during fracture healing. This broadens our understanding of the previously understudied role of vitamin B12 in bone metabolism and repair. The results point to a possible beneficial use of vitamin B12 in improving fracture healing.
The Potential Limitations of these studies include small sample Size and short period of study. The study’s statistical power is constrained by the sample size of 30 rats, of which 15 were in each group. True differences or effects may go undetected due to Type II errors, which are more likely to occur in small sample sizes. In order to produce more reliable and broadly applicable data, the ethical committee should grant future research the permission to employ a larger sample size. There was no research done on the long-term consequences, possible advantages, or disadvantages of prolonged vitamin B12 administration beyond this study size. Therefore, longer follow-up times should be taken into account in future so as to evaluate the durability of the benefits that have been seen as well as any long-term issues. Furthermore, It is possible that in this study, some confounding factors may have affected the outcomes. These factor may be age, sex, diet, genetic make-up, and general health of the rats. Aside from housing conditions, other environmental factors that may affect the results include stress management techniques. Lastly, The application of these research findings to human beings is hindered by the use of albino rats as model organisms. Since rat models are useful for initial studies, there are notable distinctions in bone biology and healing processes between humans and rats. Consequently, figuring out the practical applications of Vitamin B12 supplementation in medicine will require conducting clinical trials in humans to assess its effectiveness in fracture patients. The various forms of fractures, patient characteristics, and coexisting illnesses should all be taken into consideration in these trials.
CONCLUSION
In Conclusion, this study revealed that prolonged administration of Vitamin B12 for four weeks or more in Albino rats may enhance collagen deposition at the fracture site and potentially stimulate lamellar bone formation, thereby promoting fracture repair.
REFERENCES
- Al-Aql AI, Alagl AS, Graves DT, Gerstenfeld LC, Einhorn TA. Molecular mechanisms controlling bone formation during fracture healing and distraction osteogenesis. J Dent Res. 2008;87:107-118.
- Alejandro A, Aleksandra P, Tony C, Gideon K. Pharmacokinetics of high doses of cyanocobalamin administered by intravenous injection for 26 weeks in rats. Clin Exp Pharmacol Physiol. 2005;32(1-2):13-18.
- Aurégan J, Danoff JR, Burky RE, Akelina Y, Rosenwasser MP. The rat model of femur fracture for bone and mineral research. Bone Joint Res. 2013;2(8):149- 154.
- Bailey RL, van Wijngaarden JP. The role of B-vitamins in bone health and disease in older adults. Curr Osteoporos Rep. 2015;13(4):256-261.
- Barnes GL, Kostenuik PJ, Gerstenfeld LC, Einhorn TA. Growth factor regulation of fracture repair. J Bone Miner Res. 1999;14(11):1805-1815.
- Beamer B, Hettrich C, Lane J. Vascular endothelial growth factor: an essential component of angiogenesis and fracture healing. HSS J. 2010;6(1):85-94.
- Charles S. Fracture repair. In: Bone Regeneration and Repair: Biology and Clinical Applications. 2007:21. doi: 10.1385/1-59259-863-3:021.
- Chen Y, Whetstone HC, Lin AC, Nadesan P, Wei Q, Poon R, Alman BA. Beta- catenin signaling plays a disparate role in different phases of fracture repair: Implications for therapy to improve bone healing. PLoS Med. 2007;4.
- Clarke M, Ward M, Dickey W, Hoey L, Molloy AM, Waldron L. B-vitamin status in relation to bone mineral density in treated celiac disease patients. Scand J Gastroenterol. 2015;50(8):975-984.
- Colnot C. Skeletal cell fate decisions within periosteum and bone marrow during bone regeneration. J Bone Miner Res. 2009;24(2):274-282.
- Ebesunun MO, Umahoin KO, Alonge TO, Adebusoye LA. Plasma homocysteine, B vitamins and bone mineral density in osteoporosis: a possible risk for bone fracture. Afr J Med Med Sci. 2014;43(1):41-47.
- Gerstenfeld LC, Cullinane DM, Barnes GL, Graves DT, Einhorn TA. Fracture healing as a post-natal developmental process: molecular, spatial, and temporal aspects of its regulation. J Cell Biochem. 2003;88:873-884.
- Glatt V, Evans CH, Tetsworth K. A Concert between Biology and Biomechanics: The Influence of the Mechanical Environment on Bone Healing. Front Physiol. 2017;7:678.
- Ghiasi S, Chen J, Vaziri A, Rodriguez K, Nazarian A. Bone fracture healing in mechanobiological modeling: A review of principles and methods. Bone Rep. 2017;6:87-100.
- Halczuk K, Kaźmierczak-Barańska J, Karwowski BT, Karmańska A, Cieślak M. Vitamin B12-Multifaceted In Vivo Functions and In Vitro Applications. Nutrients. 2023;15(12):2734. doi: 10.3390/nu15122734.
- Handool KO, Ibrahim SM, Kaka U, Omar MA, Yusoff MS, Yusof LM. Optimization of a closed rat tibial fracture model. J Exp Orthop. 2018;5:13.
- Hankenson KD, Dishowitz M, Gray C, Schenker M. Angiogenesis in bone regeneration. Injury. 2011;42(6):556-561.
- Haffner-Luntzer M, Kovtun A, Rapp AE, Anita IA. Mouse models in bone fracture healing research. Curr Mol Biol Rep. 2016;2(2):101-111.
- Hulth A. Current concepts of fracture healing. Clin Orthop Relat Res.1989;(249):265-284.
- Kwon TG, Zhao X, Yang Q, Li Y, Ge C, Zhao G, Franceschi RT. Physical and functional interactions between Runx2 and HIF-1α induce vascular endothelial growth factor gene expression. J Cell Biochem. 2011;112(12):3582-3593.
- Lin H, Sohn J, Shen H, Langhans MT, Tuan RS. Bone marrow mesenchymal stem cells: Aging and tissue engineering applications to enhance bone healing.Biomaterials. 2019;203:96-110.
- Macêdo LG, Carvalho CG, Cavalcanti JC, Freitas BA. Vitamin B12, bone mineral density and fracture risk in adults: A systematic review. Rev Assoc Med Bras. 2017;63(9):801-809.
- Mana HP, Haruna AA, Abba AA, Idris MA. Management of compound fracture of the radius and ulna using pop and splints in a Nigerian Indigenous breed of dog: Case report. Int J Vet Sci Anim Husb. 2022;7(2):21-24.
- Mana HP, Hermon W, Mutah AA. Effect of prolonged administration of caffeine during fracture repair progression in rats. Int J Vet Sci Anim Husb. 2023;8(1):44-48.
- Mutah AA, Mana HP, Laku D, Mohzo DL, Ahmed II, Bolbonga G. Effect of serum hyaluronic acid on wound healing in Wistar rats. Sahel J Vet Sci. 2023;20(2):14-21. doi: 10.54058/saheljvs.v20i2.361.