
Experiences of Elderly Caregivers of HIV/AIDS Orphans in Magamba Ward in Rusape, Manicaland, Zimbabwe
- Doreen E. Kavumbura
- 1445-1461
- Feb 23, 2023
- Psychology +1 more
Experiences of Elderly Caregivers of HIV/AIDS Orphans in Magamba Ward in Rusape, Manicaland, Zimbabwe
Doreen E. Kavumbura
Intern Counselling Psychologist, Crisis Support Centre, Parirenyatwa Hospital, Harare, Zimbabwe
Abstract
The study sought to explore the psychological and social experiences of the elderly caregivers of orphans of HIV/ AIDS in a rural setting in eastern Zimbabwe and to gain insight into the nature of the coping strategies which they employ to deal with these challenges each day. A qualitative study was carried out in Magamba Ward in Rusape, Manicaland, in Eastern Zimbabwe targeting homes that have one or more HIV/AIDS orphans who were being taken care of by their grandmothers who are over the age of sixty. Twelve grandmothers were interviewed in their homes in the presence of the Village Health Worker when saturation of data was reached. Semi-structured individual interviews were used for data collection and a thematic analysis was used to identify the challenges faced by the elderly caregivers. The study revealed that of the twelve caregivers, only two had tertiary level education and none of them were employed and that the orphans were between the ages of nine and nineteen years and were still in primary and secondary schools. Seven themes which emerged from interviews were poverty and lack of money, struggles with health issues, problems dealing with rebellious teenagers, feelings of hopelessness and despondency, lack of support from Social Services and family members, dealing with stigmatization and discrimination and the overwhelming nature of the job. It was found that elderly caregivers had resorted to tilling the land in order to increase food security and overcome poverty. Sometimes they would sell the surplus to get some money to cover medical expenses and some school requirements for the children. They also relied on the grandchildren to provide physical labour to work in the fields or to work for other community members to raise money and relied heavily on their belief in God to get hope for the future.
Key Words: Elderly caregivers; HIV and AIDS; Orphans; Poverty; Stigmatization; Caregiver burden
Introduction
It has been over thirty years since the outbreak of the HIV and AIDS epidemic, which has left many families and communities in Sub-Saharan Africa, as well as Zimbabwe, devastated as millions of economically active people became infected. Consequently, thousands and thousands of deaths have been recorded yearly and many children below the age of twenty have been orphaned and left in the care of aged grandparents. Most of these grandmothers have gone past the productive stage, deprived of basic income and are without the means to sustain the lives of these orphans.
This study, therefore, seeks to examine the experiences of elderly caregivers in taking care of the children orphaned by HIV and AIDS, focusing on Zimbabwe since it is one of the countries which have recorded some of the highest HIV/AIDS statistics in the region. Due to time limitation, this study shall focus on Magamba Ward, Makoni District in Rusape which is one of the few well organised communities which are currently carrying this burden. The strategies which they are using to cope with the experience of taking care of the infected and mostly affected children will be examined.
The study by UNAIDS cited by Hope & Fraderick (2011) revealed that in 2001, of the 29.5 million adults and children who were infected with HIV globally, 20 million lived in Sub-Saharan Africa. Hope and Fraderick also mentioned that Africa was identified as the continent with the highest HIV prevalence, with 42 million people infected with the virus by 2002. Skinner, et. al (2006) pointed out that 14 million children were either single or double orphans of HIV and AIDS by 2001 and were growing up either in foster homes or living with extended families. It is within these extended families that the children are mostly taken care of by elderly caregivers, usually their maternal or paternal grandmothers. Dorrington, (2006) noted an increase of 52% from approximately 400 000 maternal or double AIDS orphans in South Africa since 2001.
Ssengonzi (2009) noted that researches which were conducted in Thailand, Uganda and Zimbabwe revealed that two thirds of the elderly respondents were the main caregivers of ill adults or orphans whose parents had died of AIDS. Howard et al (2005), reported that in Zimbabwe, where one quarter of the adults are living with HIV and one fifth of the children are AIDS orphans, AIDS and economic decline are putting a strain on society’s ability to care for orphans within their extended families. According to Howard, lack of stable care was putting thousands of orphaned children at risk of malnourishment, emotional underdevelopment, illiteracy, poverty, sexual exploitation and HIV infection amongst others. The same observation was made by Stuntzner-Gibson (1991) although his study was more to show that HIV was causing cultural, social and spiritual crises resulting in problems in families and communities. Bejane and Havenga (2013) also agreed that the orphans who are either affected or infected with HIV, require long-term psycho-social care and support which they get from the elderly caregivers who are in most cases widowed, poor and are at risk of deepening poverty.
UNICEF (2003) highlighted that most orphans are taken in by rural households which are more often than not very poor but all within the extended family safety net. However, Nyamukapa, Gregson and Wambe (2003), Zimbabwean researchers, have found that the cost of unassisted orphan care can become too high for the caregivers and communities at large. World Health Organisation (2006; 54) cited that
“Orphans care is provided mostly in circumstances of diminished or non-existent forms of external support, be it familial or state-provided.”
This is supported in another study done in Zimbabwe by Nyatsanza et.al (2000) which revealed that only 2% of households in Zimbabwe were benefitting from public education, food and health-care assistance. Without such support, given the caregiver’s illness and frailty, all these variables would make life very difficult not just for the caregiver but for the orphaned child as well. This was almost seventeen years ago and things were relative “good” in Zimbabwe.
It was also documented that there was little understanding about the kind of psychological interventions that would enhance HIV/AIDS orphan care (D’Cruz,2004). He noted that the fragmented understanding of caregiver experiences hampered the creation of effective policies and programmes, underscoring the need to address the gap. For the caregivers to provide the necessary care, they need to be provided with adequate support (Chimwaza & Watkins, 2004). This is only possible if all the stakeholders have a better understanding of the impact of the disease on the elderly caregivers and the care responsibilities that go with it. There is therefore a need to examine the impact of HIV, not only on the orphaned children, but also on the caregivers who are equally affected.
In spite of the importance of the role of the elderly in caring for the vulnerable children, the existing literature paid little attention to this population that continues to increase with escalation in the number of HIV/AIDS orphans. It seems that very little research has been done to better understand the unique experiences of the elderly caregivers given their age, health issues and economic circumstances.
So are there any possible ways in which their needs can be addressed by HIV/AIDS programmes which mostly focus on the orphans and people living with AIDS, without paying much attention to the elderly caregivers of those orphans? It is in response to this gap in knowledge that this researcher is proposing to conduct an exploratory study in Sub-Saharan Africa focusing on Magamba Ward in Makoni District of Rusape in the Manicaland province of Zimbabwe.
Because of the AIDS epidemic in African countries, adult mortality rate has increased resulting in the increased number of orphans. As a consequence, more and more grandparents are left to take care of their orphaned grandchildren. In Zimbabwe, the AIDS epidemic feeds and is fed by an economic meltdown marked by 70% unemployment (much higher by now I am sure), a shattered agricultural sector, a devastating drought, drastic reduction in social spending and political uncertainty (USAID, 2004). Research done by Dyk (2007) shows that stress manifests more strongly in the field of HIV/AIDS than in other fields because of the many factors at play like mourning for adult children who have died, nursing of adult children who are suffering from AIDS related illnesses, lack of money because of the illness and increased size of households and the associated responsibilities The same study also showed that continued exposure to the sickness and deaths from HIV/AIDS and other related difficulties further exacerbated the risk of occupational stress for AIDS orphan caregivers (Dyk, 2007). It is because of the magnitude of this problem that the researcher has decided to carry out a study to find the exact nature of the challenges faced by these elderly caregivers in taking care of their orphaned grandchildren and how they cope with the identified challenges.
Methods
The target population for the study at hand consisted of all rural female caregivers of HIV/AIDS orphans in Makoni District, in Manicaland Province in Eastern Zimbabwe. A purposive sampling technique was used to select the participants for this study. The technique was chosen because it enables the researcher to concentrate on people with particular characteristics, who are better able to assist with the research. In this study, the elderly women chosen had hands on experience caring for HIV and AIDS orphans and the information supplied was based on their lived experiences. The interviewed participants were from Bingaguru Rural Health Centre which services the area that covers villages 43 to 48 in Magamba Ward. All 12 participants took care of HIV/AIDS single and double orphans, aged between 6 and 19 years. None of the participants had received some form of training in care-giving and were not employed. Some of them lived with some of their children who were also HIV positive and were parents to the single orphans. The research study used in-depth interviews, with the aid of semi-structured questionnaires, to explore the phenomenon under investigation. Permission to access the participants at Bingaguru Rural Health Centre was sought from the chairman of Magamba Ward. All communication was done in Shona as all the people concerned could speak and understand the language well. To test for the validity and reliability of the data collecting instruments, a pre-test study was carried out using participants from Chinyika Ward which is close to Magamba Ward but was not included in the research sample. A thematic content analysis was used to analyse the research data. Research ethics were maintained during and after the research.
Results
DEMOGRAPHY OF PARTICIPANTS
The findings were based on the thematic content analysis of the interview transcripts of the participants. The results of the study are expected to answer the research questions which were the main focus of the study. The questions which were addressed were as follows;
- What are the psychological experiences of elderly caregivers within the context of HIV and AIDS?
- What are the social challenges of elderly caregivers in taking care of HIV and AIDS orphans?
- What mechanisms are employed by elderly caregivers to cope with the experiences they encounter in the execution of their duties and how can they be improved?
Table 1: Demographic Information of Participants
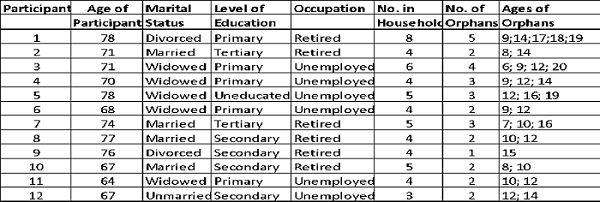
The elderly people who were interviewed were all women over the age of 60 years and they were all taking care of their grandchildren who were orphans of HIV/AIDS. Most of them had primary school education. Those with secondary or tertiary education were now retired from some government jobs, mostly teachers and others had worked as domestic workers when they were younger. The ones who said they were not employed were in fact subsistent farmers who grew mostly tobacco as a cash crop and maize for food. Some of the elderly caregivers also took care of their adult children who were widowed and in almost all the cases, the adult children were also living with HIV.
The questions on the instrument were not asked in any particular order but followed each other depending on what the respondent was talking about at that time. The researcher used the questions to guide the conversation and to make sure the respondent was not deviating from the main objective of the interview.
Table 2: Themes that emerged from the interviews

Table 2 above shows the themes that emerged from the interview transcripts. The findings of the study were presented in table form in order to show how each of the participants responded to the issues that were presented to them in the interviews.
Poverty and lack of money
The first theme that emerged from the interview transcripts was that of poverty and lack of money. The findings of the study were that the elderly headed households were very poor as most of them were not employed nor did they have any form of pension to live on. This resulted in lack of basic necessities like food, toiletries and money for transport and medicine.
The illness of the children and sometimes their parents, drove the families deeper into poverty because they used up whatever resources they had in an attempt to get those who were ill to get better. They sold their cattle, chickens and sometimes implements to raise money for medicine for those who were ill.
The majority of the caregivers reported experiencing distress and despair because they were unable to provide for their grandchildren. The families sometimes went to bed hungry and the children were the ones who suffered more than the adults because they needed balanced nutrition for optimum development. Due to lack of money, some of the children dropped out of school because their grandmothers could not afford to pay school fees and buy some school requirements like books and uniforms.
Only two of the participants did not report poverty as a major issue in their households. Participant number one looks after five HIV/AIDS orphans and one HIV positive daughter- in-law.
Participant No. 1 indicated in Table 1 above had this to say
“If it were not for my daughter and her husband who have provided for us since my two sons died, I do not know how we would have survived. They give us money for school fees, uniforms, books and even shoes for all these children. Although we grow most of our food, they buy the other food stuffs like sugar, cooking oil, rice, flour and toiletries like soap, toothpaste and petroleum jelly. We also have a lot of cattle which supply us with milk and meat. My grandchildren have had a very good life although they are orphans because their every need has been met up to now. The children are however becoming stubborn and disrespectful because they are now teenagers. This greatly disheartens my daughter who had always given them whatever they needed and it depresses me a lot”. (Participant #1, 78, interviewed at Magamba Ward, Rusape on 20 April 2017at 15h00),
Participant No. 2 did not say much about poverty but mentioned that she was a teacher most of her life and is now retired. She receives a small pension but she also reported that she had invested her salary income in real estate while she was still working. The same real estate is generating revenue which she is currently surviving on together with the two children she is taking care of.
Apart from these two grandmothers, the rest of the caregivers reported feelings of hopelessness and disappointment at not being able to provide for their orphaned grandchildren even with the most basic of necessities.
Overwhelming nature of the work
This theme is based on the expressions of the caregivers of how their work impacted on their emotional and physical functioning. The elderly grandmothers reported that they had to do many chores for the children like cooking, washing their clothes and taking them to the clinic when they were not feeling well.
Taking the children to the health centre for treatment posed the biggest challenge as there were no buses and the roads were bad. Sometimes the children contracted malaria, which is very common in their area, and at other times they got gastro-enteritis. In such cases, the caregivers had to take them to the health centre in wheelbarrows or ox-drawn carts.
The elderly caregivers were required to go with the children because the nurses at the health centre expect that children be accompanied by adults at all times. This exercise itself made the grandmothers very tired and sometimes they even fell ill. What really frustrated them most was that sometimes the health centres did not have the necessary medication and their efforts would have been in vain. The endless work they did for the orphans as well as taking care of their households made the caregivers experience both emotional and physical fatigue.
Participant No. 5, who lives with three teenage orphans sounded discouraged as she said,
“You see my fingers are all crooked and they are painful. At night I do not sleep at all because of the pain but I still have to work. All the children go to school and by the time they get back it is already dark. They also have a lot of homework. Sometimes I wish I could just sit and rest but I have to cook lunch, fetch water and do the cleaning. I wonder when all this is going to end because I really feel tired most of the time”. (Participant #5,78, interviewed at Magamba Ward in Rusape on 20 April, 2017 at 10h00).
Further, some caregivers reported feelings of hopelessness and a desire to give up and just go away from it all but then again they did not leave because there was no one else to take care of the children. These elderly caregivers seemed to be in a moral dilemma of wanting to help and at the same time wanting to abandon the children because of the never ending challenges. A significant number of the caregivers reported symptoms like lack of sleep, poor appetite, headaches and lack of motivation. These are all signs of the distress that they experienced because of the demands of their care-giving work.
Lack of Assistance from Social Welfare and family members
Another theme that emerged from the analysis of the interview transcripts was that the elderly caregivers reported that they did not receive any form of assistance from the Social Welfare arm of the Ministry of Health. These elderly ladies were aware that there is a Social Welfare Department but wondered who their beneficiaries were since they did not benefit from their services.
They believed that they should receive some form of grant for them the buy food since they were too old to work. They also knew that their grandchildren were entitled to the Orphans and Vulnerable Children’s grants but wondered why they were not receiving anything.
All twelve caregivers felt that they should receive some money from Government to take care of the orphans. They also stated that they required financial support because of the health problems of the orphans as well as their own. If the Social Welfare Department gave them some form of assistance, then they would have money to buy food and to pay for their grandchildren’s education.
One very angry caregiver had this to say about the clothes and food handouts they used to receive from GOAL, a non-governmental organisation that used to work in their area.
“We used to get food and clothes for ourselves and our grandchildren from “GO” but the ward officials started putting the names of their able-bodied relatives on the list for the handouts. The food was therefore diverted from those who needed it most and given to those who did not deserve it and they sometimes sold the food and clothes. There is a lot of corruption in this ward and that is why “Go” left. Now how can we feed these children on our own? We are not working and we cannot do business because we are old. Government must help with food so that we can feed these children. I have sold all my cattle in order to raise these children. Now I am poorer than before they came to live with us”. (Participant # 6, 68, interviewed at Magamba Ward, Rusape on 17 April 2017 at 12h00).
With regard to education of the HIV/AIDS orphans, the challenge was how to raise money to pay school fees and buy other school requirements like books and uniforms. The caregivers decried the large amounts of money required for building fund, sports fees and many different levies. They also indicated that although schools received some school fees from government through BEAM, there were delays in receiving the money and this forced the teachers to find resources from families who could not afford them. As a result, the children dropped out of school and some surveys have shown that orphans had the highest rate of school drop-out.
The impoverished caregivers felt if they received support from Social Welfare, their grandchildren would also have a chance of receiving a decent education like all other children. Most elderly caregivers who were interviewed expressed disappointment with their families because they also did not help. Although most extended families were also suffering because of the depressed economic climate, the caregivers expected to at least receive moral if not financial support. One grandmother who expressed her frustrations with family members who do not want to help said,
“If only my surviving son and his wife would sometimes visit and help me take care of the children. They just stay in Marondera where they live and seldom come to check on me and the children. I am old now and my knees are very sore but I carry on because I have no choice. If I do not do it, then who will do it? My other daughter-in-law is on ARVs and she cannot do it all by herself. She is the one who inspires me to go on because she never gives up. God bless her soul. At night I do not sleep well because of the pain in my back and my legs but when morning comes, I have to drag myself out of bed and carry on. This lack of support from family members causes me a lot of frustration”.( Participant #1aged 78,interviewed at Magamba Ward in Rusape on 20 April, 2017at 15h00.)
However, the other caregivers shared that as the children grew older, they took over some of the household chores and this brought some respite to the grandmothers. The boys took over manly jobs like collecting firewood, herding cattle when they were not in school as well as ploughing the fields. The girls cooked, cleaned and did the washing in the nearby Chinyika river. In some households where the caregiver had become too frail to do most of the chores, girl children were made to drop out of school to assist in the home which is not necessarily a good thing because this perpetuates the cycle of poverty and hopelessness.
Failure to discipline rebellious orphans
The caregivers’ inability to discipline their orphaned grandchildren was one theme that emerged very strongly from the interviews. All the caregivers reported that as the children in their care grew older, they became more and more stubborn. The children did not listen to their grandmothers and some of them even engaged in questionable behaviours like drinking, smoking and promiscuous sex. The elderly caregivers find it challenging to care for such children, especially adolescents. The grandmother of five orphans, four of whom are now adolescents and live in her household, said;
“Now that these four are teenagers, they just do what they want and their mother and I are finding it more and more difficult to instil discipline in these children. One time the mother tried to discipline her older son who is now seventeen and he simply challenged her to try it. The mother became scared and left him alone. We have also noticed that these days if one leaves money in the bedroom, it simply disappears and no one ever owns up to taking it. It is a bad habit that has invaded this home but we still do not know who is responsible for the theft. And one of the girls spends too much time outside the home and if you ask her she always says she was looking for a spot where she can get network for her phone. I hate these “cellphones” and this business of “whatsapp”. No one does any work anymore because of “whatsapp”. Some people in the village have told us that this girl is always seen with boys or even older men. I think she is sleeping around but what can I do since I cannot even walk properly. This really depresses me because I think these children do this because there is no man in our household. Tell me what am I supposed to do with these children? Is it wrong that I gave up my own desires so that I can look after them and give them a chance of a better future? One day I will just go away and leave them here”. (Participant #1, 78, interviewed at Magamba Ward, Rusape on 17April, 2017 at 15h00).
Another caregiver who is unmarried and takes care of two AIDS orphans, one of whom is living with HIV expressed disappointment at her granddaughter who contracted HIV from sleeping around and said that;
“This girl is really a disappointment. I was doing all I could so she could carry on with her education, then she ran away from home. She is on ARVs and I worry that wherever she is maybe she is not even taking her medication. I do not know what else to do except pray to God that He keeps her safe”. (Participant #11, 64, interviewed at Magamba Ward in Rusape on 17 April,2017 at 11h00).
The saddest story which I heard during the interviews from the caregivers was about a seventeen -year- old girl who had HIV from birth. It was revealed that she had been on ARVs all her life and she had been doing well until she turned fifteen years of age. At that age, she decided that she did not want to take her medication any longer. The grandmother tried to explain the consequences of not taking her medication but she did not care because she could not have a boyfriend like other girls because of her status. The researcher later gathered that the girl had passed away. Non-compliance among teenagers was reported to be very high and it was a major problem for the grandmothers because they did not know how to deal with the teenagers especially where discipline was concerned. Only participants 3, 8 and 11 did not report discipline problems mainly because their grandchildren were not yet at the adolescent stage.
Feelings of hopelessness and despondency
All twelve elderly caregivers expressed a sense of hopelessness given the nature of their work and their age. The elderly caregivers reported that they viewed their situation with the orphans as pretty hopeless as they did not see a bright future for their grandchildren. In most cases they reported that the extended family did not want to be involved in the welfare of these children. One grandmother expressed concern over the children’s lives later on in life as she had this to say;
“As you can see, I am already 78 years old and I can hardly walk. Right now we manage to grow food for ourselves because I keep telling the children what to do. I tell them to plough the fields when it’s time, to sow vegetable seeds in the garden and to take care of the cattle and goats. It is like I am the brain behind everything that goes on here. I cannot even visit my sister who is always inviting me to go and visit for a while because I fear what might take place in my absence. Now when I die who is going to do all that? I feel so helpless because I do not see a bright future for my grandchildren. The youngest is nine years old. What is going to happen to him? The others are a bit older but they are all still teenagers and they are not very good in school. If at least one of them could get a decent education and then a job, then they can take care of each other. There is not a day that I do not worry about the future of these children after I am gone. It gives me sleepless nights and sometimes I feel depressed because there seems to be no way out. If only our government could assist by having grants for orphaned children, then they could manage on their own. Now, without any source of income I worry that they will end up doing illegal things like stealing and prostitution and end up in jail. Right now all I do is to pray to God to give me a few more years so that these children will be a little bit older when I die”. (Participant #1, 78, interviewed at Magamba Ward in Rusape on 17 April,2017 at 15h00).
All the caregivers who were interviewed expressed the hopelessness of their situations because they all felt that they did not have much life left in them and what they were offering to their grandchildren was not going to last forever. Their greatest fear was what was going to happen to these children who did not have anyone else except them when their grandmothers died. The depression that enveloped these elderly caregivers could be felt when they talked about their own death and the welfare of the children after their death.
Isolation, Stigmatisation and Discrimination
The findings of the study revealed that the elderly caregivers suffered from social isolation, fear of stigmatisation and discrimination. Some community members did not wish to be associated with them because their children had died from AIDS. There was always the belief that those who had died of AIDS had been promiscuous that was why they contracted the disease. One participant indicated that she felt ashamed wherever she went and people did not want to eat her food lest they contracted HIV. This was due to the fact that her daughter had died of AIDS and she was guilty by association. She reported that she was not allowed to help at community functions like weddings or funerals because the other community members thought that she was HIV positive. She went on to say;
“As a result of this discrimination and stigmatisation, I feel that it is better for me not to attend community functions. This makes me very sad because I feel lonely and isolated. Even my friends do not want to spend time with me anymore. I therefore fill my time attending to my grandchildren’s needs but it does not take away the desire to spend time with other adults. Maybe we should form an association of carers of HIV/ AIDS orphans in our ward. I think there are others out there who feel the same way I do”. (Participant #11, 64 interviewed at Magamba Ward, Rusape on 17 April. 2017 at 11h00).
Two of the participants did not report any discrimination or stigmatisation in their communities. They reported that within their communities, most people were beginning to understand that people can and will live positively with HIV. They reported that these days, people living with HIV collected ARVs from the local health centre and many people were now open about their HIV status. In these communities it was reported that there was no need to fear those who were living with HIV as they could live for a long time just like other people with chronic conditions like high blood pressure and diabetes.
Health Challenges of the Elderly Caregivers
Because of their age, the findings were that all the elderly caregivers reported some sort of health problem or other. Their ailments ranged from stiff muscles, painful joints, difficulty with mobility, high blood pressure, poor vision and whatever else comes with old age. One elderly lady reported that she spends most of her time lying on her tummy. She had this to say;
“For a long time now, when I am at home, I spent most of the time lying on my stomach. This is because I cannot sit up for long since my back is very sore. I have not been to a doctor because I do not have the money to go to Rusape or to pay the doctor. I just carry on but I cannot do much work as a result. I am glad my unmarried daughter stays with us but she is sickly as well but the pills help her a lot”. (Participant # 4, 78, interviewed at Magamba Ward, Rusape on 17 April, 2017 at 13h00)
Sickness is very common amongst the elderly caregivers but because of poverty they hardly go to hospital. The rural health centre is far from all these villages and there are no buses or commuter “taxis”. Only the young and strong, walk the five kilometres or more to go to the health centre. When the elderly become very sick they are taken in oxen-drawn carts which themselves are not very comfortable and could make them worse by the time they arrive at the health centre. The negative and arrogant attitude of some of the health care providers forces the elderly to choose not to go to hospital. They would rather go to traditional and faith healers for portions and prayer. Sometimes the health centre does not have the right medications for the ailments and they end up giving everyone with whatever ailment “panado”, the universal treatment for all illnesses.
Coping Strategies
In the face of the many challenges encountered by elderly caregivers in their everyday work, they reported that they had come up with some strategies that help them cope.
These strategies by no means answered all the problems of the elderly headed households but they brought about some respite in otherwise desperate situations.
To address the challenges of poverty and food insecurity, most households engage in subsistence farming. Those caregivers, who were still strong enough to work the land, reported that they grew tobacco for sale to raise much needed cash. This brought in some money but it was a lot of hard work since tobacco farming is labour intensive and tobacco is a long season crop. Those who grew it ended up with backache, sore joints and other old age challenges but they still carried on. Those who did not have strength to do tobacco farming only grew maize and other food crops so they could have something to eat. The grandchildren were very much involved in the work in the fields since they are the stronger ones in the families. Some even helped other members of the community in their fields or herding cattle in exchange for food or money.
When asked how they got rid of emotional challenges and stress, most of the elderly caregivers indicated that they prayed or went to church as a coping strategy. Religion emerged as an important source of emotional and spiritual strength among the elderly caregivers. All of the caregivers who were interviewed said they belonged to one or other of the many churches in the community and they acknowledged their belief and trust in God helped to improve their situation. They also encouraged the children in their care to pray and to go to church. One grandmother said
“When I feel stressed, I just go into my bedroom and pray. I like singing, so I sing church songs and that is how I forget my problems. Sometimes we sing together as a family and we have fun. The children like to sing and dance like they see others do when they go to church”. (Participant # 2, 71, interviewed at Magamba Ward, Rusape on 17 April 2017 at 15h00).
Another elderly caregiver who believed that God is their provider had this to say
“We praise God and put all our needs before Him. God will not forsake us and will give us something no matter how small. Sometimes we do not even know what we will eat and then suddenly someone just brings some mealie-meal or beans. The community members around here help each other out and we are grateful.”
Discussion
Demographic Profile
In recent years HIV infection is no longer considered a terminal illness because of the advanced medical research and the effectiveness of antiretroviral treatments. Instead, it is now regarded as a chronic illness that people can live with as long as they adhere to the treatment protocols prescribed by the health care practitioners. In spite of this medical achievement, research shows that HIV/AIDS continue to affect many sub-Saharan communities and families and Zimbabwean households are no exception. Many of the affected households are headed by elderly grandparents, mostly grandmothers over sixty years of age. The elderly grandmothers find themselves raising grandchildren orphaned by AIDS as indicated by Kuo and Operario (2009) and in addition to care-giving, they also live with poverty, financial, emotional, psycho- social and discriminatory consequences (Smith, Fawzi, Eustache, Oswald, Surkan, Louis, Scanlan, … & Mukherjee, 2010).
Before the arrival of HIV and AIDS, Zimbabwe’s culture of filial obligation allowed the elderly to depend on their grown children for financial and psychosocial support, but because these are the people dying from AIDS, if help is needed, it comes from other family members who themselves wish they could get outside help. Other sources of help are NGOs and FBOs but they generally help the orphans, if at all, leaving out the elderly caregivers (Hawkins, 2013). From the limited research focusing on the elderly caregivers, it was not very clear what the experiences of elderly caregivers in rural Zimbabwe were. The studies available in the literature focused more on the AIDS orphans and People Living with HIV/AIDS rather than the caregivers. This study was therefore carried out to try and fill this gap in literature by exploring the lived experiences of the elderly caregivers of HIV/AIDS orphans in Magamba Ward in Manicaland, Zimbabwe.
The study confirmed that Zimbabwe’s rural elderly women are the main caregivers to their grandchildren orphaned by HIV and AIDS. Even those children who used to live in the cities with their parents were brought to the rural homes after the death of their parents because there was no one to take care of them in the cities.
This study found that lack of educational, economic and social resources for caregivers and their families caused short and long-term consequences for all involved. The next paragraphs in this chapter will discuss the findings of the study and draw parallels with findings from other related studies found in the literature.
Poverty and Lack of money
If one were to take a tour of the rural Zimbabwe, one thing that would strike them even without going into any one homestead, is the poverty that surrounds the villages. Just driving past most rural homes one cannot but wonder how the people who live there manage from day to day. Dilapidated huts, unfenced homesteads, children walking to school barefoot and old grandmothers tilling the land are a common sight in rural Zimbabwe. This is the “normal” life in rural Zimbabwe, a life of poverty. It was in such a setting that the current study was carried out and poverty was one constant in all the interviews that were done.
Not surprisingly, from the findings of the current study, poverty and lack of money came out as common causes for distress among the elderly care-givers affecting their emotional well-being. Most households were very poor as the elderly were the least economically productive in society and they were not employable. The caregivers’ reports in this study were similar to the findings presented by Dyk (2007) who reported that economic constraints were a serious challenge for caregivers working in the field of HIV/AIDS. Some researchers like Lehmann and Zulu (2005), UNAIDS (2000), (Guqa,2013), Hlabyago and Ogunbanjo (2009) and Tladi (2006) have also emphasized the devastating effects that poverty has on caregivers working with those infected or affected by HIV/AIDS. Poverty and lack of money cause many other hardships like food insecurity, lack of proper clothes, inability to attend school and general state of low self- esteem and poor mental health.
Other studies carried out in the past have shown that the increased cost of health care and debts that the elderly incurred during the illness of their children and grandchildren, drove these households deeper into poverty (Ssengonzi, 2009). Related existing studies have also documented that the elderly caregivers had to meet transport costs for ailing grandchildren (Lekalakala-Mokgele, 2011), (Schatz & Ogunmefun 2007). This sentiment was echoed by the findings of this study. Also reported elsewhere in the literature is the fact that the poverty had been exacerbated by the fact that extended family members were not able to help the elderly caregivers with financial support (Lekalakala-Mokgele, 2011) because of the harsh economic conditions that were affecting most sub-Saharan Africa (Kaseke & Gumbo, 2001: 51). In Zimbabwe, a lot of families are receiving food aid because of the drought that has hit Southern Africa for the past few years. That, coupled with cash shortages, make the situation unbearable for most families and even worse for the elderly female headed households which are the subject of this study.
Another point that came out of the present study was the lack of inheritance for the AIDS orphans. Most of the elderly grandmothers shared that most of their deceased children were not employed or were self-employed so there was no pension or inheritance to talk about. (Zerubabel, 2014) cited Alpaslan and Mabutho’s (2007) report that pointed out that the elderly caregivers were left with no inheritance from the deceased parents of the AIDS orphans in their care. This is similar to the research findings mention at the beginning of this paragragh.
Poverty and lack of money meant that the elderly female-headed households had to do without some basic necessities like food and clothing. The community leaders interviewed in one study attributed shortage of food to chronic poverty which affected people’s agricultural activities in some parts of Zimbabwe (Gomba, 2011 and Ngwerume, 2005) cited in Hlatywayo, Zimondi and Nyatsanza (2015). When there is no money to buy agricultural inputs like maize seed and fertilizers, the crops fail, resulting in food insecurity. World Health Organisation (WHO) (2010) also pointed out that,
“generally the caregivers were unable to meet the conventional requirements standards for feeding the children especially in most of the developing countries due to the chronic poverty they are subjected to.”
Poverty, lack of money and the ensuing food insecurity, were reported in literature as prevalent in elderly female-headed households and the care giving responsibilities exacerbated the already compromised nutritional status of the elderly and sickly grandchildren (Charlton & Rose 2001; Nyanguru 2003; Mba, Addico& Rose 2007). This is very true of Zimbabwean rural communities and the poverty and lack of money that the elderly caregivers interviewed in the current study spoken about, are very real and strongly supported by the review of other related studies.
Overwhelming Nature of their work
With reference to the overwhelming nature of the work that the elderly caregivers did with and for the orphaned grandchildren, the study found that the caregivers sometimes experienced frustration, a desire to give up and lack of motivation. This was mainly because of the never ending challenges and inadequate rest which their frail bodies get. A significant number of the elderly caregivers who participated in the study reported that they suffer from lack of sleep, poor appetite, headaches and again lack of motivation. These are all signs of distress which is brought about by the demands of care-giving.
This was supported by findings from studies by Boon, James et al., 2010; Oburu et al., 2005; Ssengozi, 2007 which all concluded that elderly caregivers suffer from psychosocial distress as a result of the overwhelming nature of their work. Some of the caregivers find themselves in a moral dilemma of wanting take care of their children’s children but the work is too hard for them they just want to give up. For those elderly caregivers whose grandchildren are infected with HIV, they have to make sure that the children are taken to the health centre for their monthly check-ups as well as get their medication and this is not always possible because of the cost involved and the poor health of the grandmothers.
This compromises adherence because the children will miss treatment and may become ill. A study carried out by Skovdal, Campell, Madanhire, Nyamukapa and Gregson in Zimbabwe in 2011, found that adherence of children to ART was greatly compromised by the grandmothers’ inability to abide by the requirements of the regime. They mostly could not remember the review dates for the children or they could not take the children back to the health centre because of their own health challenges. This is what the grandmothers in the current study found overwhelming. Much as their hearts were willing, their bodies could not meet the demands of their commitment.
Another aspect of the work of the elderly caregivers that they found overwhelming was how to deal with the emotional needs of the orphaned grandchildren. When the parents of these children passed on, both the caregivers and the care receivers were affected emotionally. The caregivers mourned for their children while the children mourned for their parents. The caregivers reported that they found themselves at a loss for words to comfort the children. It was at this point they would appreciate support from social workers and other workers in the help professions because they would know what to say to both the children and the care-givers. Most of them ended up doing nothing because of ignorance on how to handle such situations.
A study by Hlatywayo, Zimondi and Nyatsanza (2015), revealed that the elderly caregivers reported that they resorted to strategies like drinking, scolding the children or simply keeping quiet. This was a clear indication that when it came to psychosocial support and emotional care, it was generally acknowledged that the care-givers lacked knowledge.
This finding also supported what was found by Tigere (2006), who revealed that most Orphans and Vulnerable Children, who include HIV/AIDS orphans, suffered from psychosocial and emotional challenges because their care-givers were not equipped to holistically provide for all their spiritual, mental and social needs. All this lack of knowledge, support and uncertainty adds to the overwhelming nature of the work of the elderly caregivers.
Lack of Assistance from Social Welfare and Family Members
As we all know that Zimbabwe is not a welfare state, the burden of caring for orphans of HIV/AIDS falls on their immediate families. This lack of assistance from Social Welfare and in most cases family members, was a cause for concern amongst the elderly caregivers interviewed in this study. Carrying out such a financially and emotionally demanding job, in harsh economic conditions, with little or no support from outside, was a great stressor for the elderly caregivers of HIV/AIDS orphans. The traditional support system for the elderly was destabilised (Schatz, 2007) because the reproductive and economically active section of the population was the one that HIV/AIDS attacked, leaving elderly female-headed and child-headed families. (Makiwane et al 2004; AVERT 2009; Schatz &Ogunmefun 2007).
The son who used to send money for sugar or the daughter who used to buy clothes for her mother were the ones succumbing to HIV/AIDS and left their children to be cared for by the grandmother. Other studies by Wiegers, Curry, Garbero & Hourihan (2006) have also shown that elderly-headed families could not cope with the increasing number of orphans created by HIV/AIDS and social networks had virtually collapsed due to the pressure of having to support AIDS orphaned children (Halkett, 2000; Cohen, 1998) as cited in (Lekalakala-Mokgele, 2011). All this literature highlighted the need for financial and emotional support for the elderly caregivers in order for them to carry out their obligations without additional stress.
Mudavanhu, Segalo, & Fourie (2008), reported that in some areas in Zimbabwe, grandmothers relied on aid from Non-Governmental Organisations but for the elderly in Magamba Ward and their grandchildren, such assistance stopped a long time ago. In most Wards, government and NGO assistance was not separated from political affiliation and who received assistance and who did not, was decided by the dominant party in that area and one’s political affiliation.
Lack of emotional support from family members had a negative impact on the well-being of these elderly caregivers and this came out strongly from the findings of the current study. Emotional support had been reported to be vital in assisting the caregivers in coping with the overwhelming nature of their work and it served as a buffer against stress. Held & Brann (2007), in their study on recognising stressors in HIV/AIDS volunteers and their need for support, concluded that support was the strongest variable influencing the efficacy and performance of HIV/AIDS volunteers. Dealing with children or adults infected or affected by HIV/AIDS seemed to bring about a special kind of stress that is not found in any other situation. Even Social Workers who were supposed to support and encourage the elderly caregivers in areas where they volunteer in the stress laden field of HIV/AIDS, were not visible to those who needed them most, in Magamba Ward. The lack of adequate support suggested that the elderly caregivers were never really able to deal with the emotional and mental exhaustion that they experienced every day.
In the current study, the elderly caregivers blamed the lack of financial support from government for their grandchildren’s failure to go to school. They all reported that their grandchildren did not get to stay in school because they failed to raise money to pay school fees and buy other school materials required by the schools. Mudavanhu, D., Segalo, P., & Fourie, E, 2008 also echoed by saying,
“Inadequate funding and delays in receiving school fees and BEAM budgets from government caused teachers to demand resources from families, many of whom could not afford them and as a result children dropped out of school”.
Their survey also showed that orphaned children had a higher rate of school drop-out confirming the findings of the current study. Some children dropped out of school to help out at home because their elderly caregivers could not cope with the demands of the job.
Failure to discipline rebellious orphans
Another finding of the study under discussion was that one other major stressor in the elderly grandmothers’ lives as care-givers to their HIV/AIDS orphaned grandchildren was their inability to discipline their adolescent grandchildren. In this study, nine out of the twelve participants complained about how badly the grandchildren behaved as soon as they reached puberty. The three who did not complain looked after grandchildren who were still under thirteen years old. The grandmothers reported that as the children grew older, they became more and more stubborn. They did not listen and they engaged in all sorts of undesirable activities like drinking, smoking and promiscuous sex. The elderly grandmothers said they found this very challenging because they did not have the skills to discipline these children. This finding was the same as that found in a study by Juma, Okeyo and Kidenda (2004) in Kenya. Their study revealed that many caregivers lacked skills for disciplining children and as a result they overindulged them for fear that they might run away or become depressed. The same study showed that some elderly caregivers punished the children excessively or just ignored them hoping they would change.
Hlabyago & Ogunbanjo (2009), in their study carried out in the North West Province of South Africa, also supported this finding. In their study they found that six out of the nine participants interviewed, reported frustrations of coping with rebellious orphans. There was shared concern that the orphans did not want to do anything and punishing them was like the caregivers did not love them. Some of the children had dropped out of school and those who still attended school were not performing well. This was hurtful to the caregivers and they did not know how to deal with the rebellious orphans in their care.
Disciplining orphaned children was a major challenge for elderly caregivers because they did not know how to do so correctly, it was either too little or too much. I suppose like any other parents of teenagers, the elderly did not know which method would be most effective in disciplining their grandchildren. Those of us who have raised children, can also identify with the challenges of trying to discipline teenagers. One does not know whether dialogue, withdrawal of privileges or downright screaming contest would achieve the desired results. If biological parents face such challenges, what more frail grandmothers who are not even their parents.
Isolation, Stigmatisation and Discrimination
Isolation, stigmatisation and discrimination were found to be like a common thread amongst all except two of the participants in this study. What caused isolation in almost all cases was fear of stigmatisation and discrimination because of their association with their deceased children who had died from AIDS related illnesses and their grandchildren who were HIV positive, in some cases. Some caregivers revealed that they would rather stay away from community functions for fear of the treatment they would receive from community members who would insult them and their grandchildren. Most of the reactions were a result of ignorance or little information concerning HIV/AIDS and how they are transmitted. A study by Lekalakala- Mokgele (2011), revealed that a major psychological impact of HIV/AIDS on the elderly was the reduced participation in social activities, since they feared negative community reactions towards the children in their care who were living with HIV.
The children also had to deal with the stigma attached to and often the irrational fear surrounding AIDS (Alpaslan & Mabutho, 2005:277) cited in Lekalakala- Mokgele (2011), In general, the psychological health and well-being of the elderly has been reported to be worsening because of dealing with HIV/AIDS that was affecting their loved ones and the shame that they had to live with because of the stigma surrounding them. All these issues that impacted negatively on the mental health and well-being of the elderly caregivers were confirmed by the findings of the current study and other related studies in the literature.
Caregivers Health Challenges
Last but not least we will look at the health challenges experienced by the elderly caregivers in this study and what related studies in the literature contribute on this issue. The elderly caregivers in this study reported that they suffer from many different ailments but they did not put too much emphasis on this because they were more concerned about the health issues of the orphans and how to get them to the health centre in the face of their poverty and other logistic challenges. However, most of them confessed that they have joint pains, diabetes and hypertension which in most cases went untreated because whatever little resources they had, they spent on the grandchildren. Ssengonzi (2007) pointed out that,
“The physical impact of caring for the ill, such as backache, chest and leg pains, was attributed to the frequent changing, lifting and washing of adult patients”.
Most of these ailments would have been acquired when the elderly caregivers were still looking after their diseased children, the parents of the orphans, before they died. This revealed that these elderly caregivers were first caregivers to their adult children who were ill from HIV/AIDS and then after they died, the grandparents took over the duty of looking after their orphaned grandchildren. This revelation means the elderly caregivers’ health problems started long before they took over the children. The work of providing for the children had made their conditions worse as now the work load had increased with three or four children added to their households.
Some of the participants who were interviewed in this study revealed that they suffered from headaches, arthritis, poor circulation and sometimes even depression. These ailments were mostly due to stress that the elderly caregivers experienced because they were always worrying about not being able to provide adequate food and clothing for their families, and also how they were going to raise money for health care and school supplies. This was documented in the literature by AIDS Alliance (2007). (Juma, 2004) in another study in Kenya, confirmed that old age and ill health limited the elderly caregivers’ capacity to perform their care-giving activities. They were reported to often complain of debilitating ailments such as backache, joint aches, high blood pressure and mobility problems. These ailments were almost the same as those reported by some of the elderly grandmothers interviewed in Magamba Ward in Manicaland. This showed the universal nature of the challenges experienced by elderly caregivers of HIV/AIDS orphans in sub-Saharan communities in Africa. Whether one was in Zimbabwe, Uganda or Nigeria, the challenges remained the same.
Coping Strategies
In the face of perennial poverty and lack of money, many households have had to come up with some strategies to survive in a harsh economic environment. From the findings of this study a few coping strategies were picked up. To counter the ravages of poverty and food insecurity, most elderly caregivers reported that they engaged in subsistence farming to grow their own food. Those elderly caregivers who still felt strong enough to work their land, even grew tobacco for sale in order to raise much needed cash for school requirements and healthcare expenses for their grandchildren. The grandchildren supplied most of the labour as they were the stronger ones compared to their grandparents.
Contrary to the belief that the children come to these households as burdens, some studies have highlighted the reciprocal nature of the relationship in terms of care and support within such households (Skovdal, 2010) These studies pointed out that although the elderly guardians provided the HIV/AIDS orphaned children with a home and a place to belong, their old age, illness and fragility limited their contribution towards income and food generation. This meant they depended on the contribution and active participation of the children in sustaining their livelihoods (Skovdal, 2010) and in some cases health (Skovdal et al, 2009). This study echoed what some of the participants in the current study had to say about their grandchildren. They reported that as the children grew older, they took over some of the household chores. The boys were reported to take over the manly jobs like collecting firewood, herding cattle as well as ploughing the fields during weekends and school holidays while the girls cooked, cleaned, did the washing in the nearby Chinyika river, and helped with weeding. This strategy worked for many households as they did not have to depend on handouts or even go hungry. Hlatywayo, Zimondi and Nyatsanza (2015), in their study “Challenges of coping with orphans and vulnerable children at household level” in Gutu district, Masvingo Province, also confirmed this finding. They supported the finding that agriculture was the major activity that the elderly caregivers engaged in to alleviate poverty, food insecurity and the lack of money. They even mentioned that some of the orphans sold their labour to their neighbours in exchange for money to buy some basic necessities for their impoverished households.
Another coping strategy that was common among the elderly caregivers who were interviewed was praying and attending church. Religion emerged as an important source of emotional and spiritual strength for the elderly caregivers. Even the study done by Juma (2004) mentioned that most caregivers used their belief in God as a coping mechanism and they believed that indeed God answered their prayers and provided for them in desperate times. This strategy helped the elderly caregivers handle their emotional challenges and stress with hope.
Traditional leaders were also found to be pillars of support for the elderly caregivers as they offered guidance and counselling both to the elderly caregivers and their grandchildren. One elderly caregiver in the study conducted by this researcher mentioned that when she was stressed by the disobedient orphans, she sought the counsel of the Village Chairman who in some instances offered to discipline the children, especially the boys, on her behalf.
The study findings were that sometimes NGOs like GOAL have supplied food and school requirements to the elderly headed households to help reduce the burden of care from the already overwhelmed caregiver grandmothers. Reliable sources have however reported that this was no longer the case because the policies at government level did not support NGOs working directly with people at grass-root level. Another way that has helped the elderly caregivers to keep their grandchildren clothed was to buy most of their clothes from the flea markets where all sorts of second-hand merchandise was sold for very little. This strategy has kept many children as well as adults in elderly headed households clothed.
Limitations
The major limitation of this study was that the study used a very small sample of twelve participants drawn from the same community, Magamba Ward in Rusape, Manicaland. This makes it difficult to make generalisations about the psychological and social experiences of elderly caregivers of HIV/AIDS orphans. A larger scale study would have allowed for more generalised findings.
Another limitation of the study was the exclusion of male participants from the study. The researcher made the assumption that only elderly females were the caregivers of HIV/AIDS orphans at household level. Future studies should make an effort to include elderly male caregivers if they could be found.
Conclusion
This study set out to investigate the lived experiences of the elderly caregivers of HIV/AIDS orphans in Magamba Ward in Manicaland Province in eastern Zimbabwe. These lived experiences included the psychological and social experiences that the elderly caregivers had to deal with in their everyday work and the mechanisms they employed to cope with challenges that arose in their line of duty.
The study indicates that older people were playing major care-giving roles whilst facing many challenges that included limited resources, knowledge, skills and social support. The elderly caregivers also lacked welfare and emotional support from families in their care of HIV/AIDS orphans.
To sum it all, it is fitting to say the results of the study indicate that caring for HIV/AIDS orphans could be emotionally, mentally and physically challenging. It was only because of the love for their grandchildren that the elderly caregivers often came up with coping strategies that made it possible for them to soldier on in spite of all the challenges.
This study adds to the body of knowledge in the field of HIV/AIDS and seeks to inform policy makers and organisations, especially government organisations and NGOs with the hope that they could bring much needed positive change to the experiences of elderly caregivers of HIV/AIDS orphans, especially in rural areas of sub-Saharan Africa in general and Zimbabwe in particular.
References
- Bejane, S. M., E. Van Aswegen, and Y. Havenga. (2013). Primary caregivers’ challenges related to caring for children living with HIV in a semi-rural area in South Africa . Africa Journal of Nursing and Midwifery, 15.1 (2013): 68-80.
- D’Cruz, P. (2004). Family care in HIV/AIDS: Exploring lived experience . India: SAGE Publications.
- Guqa, V. V. (2013). The psychological impact of caregiving on carers of HIV/AIDS orphans . Doctoral dissertation.
- Held, M. B. (2007). Recognizing HIV/AIDS volunteers’ stressors and desire for support. Aids Care, 19(2), 212-214.
- Hlabyago, K. E., & Ogunbanjo, G. A. (2009). The experiences of family caregivers concerning their care of HIV/AIDS orphans. . South African Family Practice, 51(6), 506-511.
- Kuo, C., & Operario, D. (2009). Caring for AIDS-orphaned children: A systematic review of studies on caregivers.Vulnerable Children and Youth Studies, 4(1), 1-12.
- Lekalakala-Mokgele, E. (2011). L. A literature review of the impact of HIV and AIDS on the role of the elderly in the sub-Saharan African community: review article. Health SA Gesondheid, 16(1), 1-6.
- Juma, M., Okeyo, T., & Kidenda, G (2004). ? Our hearts are willing but?”. Challenges of elderly caregivers in rural Kenya.
- Makadzange Kevin (2011). The challenges of elderly caregivers who look after HIV positive orphans on ARVs in Swaziland.
- Mudavanhu, D., Segalo, P., & Fourie, E. (2008). Grandmothers caring for their grandchildren orphaned by HIV and AIDS. New Voices in Psychology, 4(1), 76-97.
- Nyamukapa, Constance, Simon Gregson, and Mainford Wambe. (2003). Extended family childcare arrangements and orphan education in Eastern Zimbabwe . scientific meeting on empirical evidence for the demographic and socio-economic impact of AIDS, hosted by HEARD.
- Schatz, E., & Ogunmefun, C. (2007). Caring and contributing: The role of older women in rural South African multi-generational households in the HIV/AIDS era. World Development, 35(8), 1390-1403.
- Skovdal, M. (2010). Children caring for their “caregivers”: Exploring the caring arrangements in households affected by AIDS in Western Kenya. AIDS care, 22(1), 96-103.
- Ssengonzi, R. (. (2009). The impact of HIV/AIDS on the living arrangements and well-being of elderly caregivers in rural Uganda. AIDS care, 21(3), 309-314.
- Stuntzner-Gibson, D. (1991). Women and HIV disease: An emerging social crisis. . Social Work, 36(1), 22-28.
- UNAIDS and UNICEF (2004) Children on the Brink 2004: A joint report of New Orphan Estimates and Framework for Action, UNAIDS, New York: USAID; 2004. Retrieved from http://apps.who.int/globallatlas/predefinedReports/EFS2008pdf.
- WHO (2002). World Health Organisation. Active Ageing: A policy framework, WORLD Health Organisation, Non-communicable Disease Prevention and Health Promotion, Aging and Life Course.
- Wiegers, E., Curry, J., Garbero, A., & Hourihan, J. (2006). Patterns of vulnerability to AIDS impacts in Zambian households.,. Development and Change, 37(5), 1073-1096.
- Zerubabel, E. (2014). A Study of the Life Condition of Older Caregivers to their Grandchildren Orphaned due to HIV/AIDS in Kolfe Keraniyo Sub-City, Addis Ababa . (Doctoral dissertation, AAU.