
Voluntary Medical Male Circumcision Service Provision by Female Nurses: Assessing Locals’ Perceptions and Attitudes in Homa Bay County
- Feddis Mumba
- Chrispine O. Ngwawe
- 2262-2272
- Aug 2, 2024
- Education
Voluntary Medical Male Circumcision Service Provision by Female Nurses: Assessing Locals’ Perceptions and Attitudes in Homa Bay County
Feddis Mumba, Chrispine O. Ngwawe*
Great Lakes University of Kisumu, Kenya; Maseno University, Kenya
*Corresponding Author
DOI: https://dx.doi.org/10.47772/IJRISS.2024.803165S
Received: 20 May 2024; Revised: 04 June 2024; Accepted: 06 June 2024; Published: 02 August 2024
ABSTRACT
Introduction: The Human Immune Deficiency Virus (HIV) pandemic is among the critical public health challenges facing the world especially the African continent today, and success in this setting remains critical in stemming this global epidemic. Kenya launched voluntary medical male circumcision (VMMC) programme in 2008 that proved successful in reaching a large population of uncircumcised men and is associated with substantial reduction in the transmission of HIV. However, Homa Bay County, Nyanza region still reports low circumcision rates and high HIV prevalence compared to the neighbouring counties like Migori at 52.6% and with Homa Bay at 26.7% of voluntary male circumcision rates
Objectives: The study sought to determine the influence of locals’ perceptions and attitudes on the acceptability of female nurses in the provision of VMMC services in Rangwe Sub-County, Homa Bay County.
Methodology: Study population was circumcised and uncircumcised men aged 18-50 years seeking services in eight selected health facilities in East Gem Ward, Rangwe Sub- County, Homa Bay County. The Fisher formula was used to sample respondents for the study. Descriptive study design was used. Both inferential and descriptive methods were used in the data management.
Results: Revealed that MMC being freely discussed at the workplace or in the community had a statistically significant association with acceptability of female nurses in the provision of VMMC services (p = 0.000). This shows that a significant majority (89%) of the respondents whose places of work or community freely discussed VMMC, compared to 57% of the respondents whose places of work or community did not freely discuss VMMC, would recommend that female nurses be trained on VMMC and be allowed to provide the VMMC services. However, the attitude of the respondents’ workmates or community had no statistically significant association with acceptability of female nurses in the provision of VMMC services [c2(3) = 7.661, p = 0.054]. In other words, there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents whose places of work or community freely discussed VMMC and those whose places of work or community did not freely discuss VMMC.
Conclusion: This is one among the few studies that focused on the acceptability of Female Nurses in the provision of voluntary medical male circumcision (VMMC) services despite the fact that male circumcision is one of the oldest and most common surgical procedures practiced worldwide performed by trained doctors, nurses and clinical officers, and traditional circumcisers in some communities. Many studies on male circumcision did not specifically dwell on acceptability of circumcisers based on their gender.
Therefore, Ministry of Health and the County government of Homa Bay should develop appropriately tailored messages for communities to use as they engage in discussions on VMMC by female nurse at workplaces and in the community to help in decision making on policy change regarding the involvement of female nurses in VMMC service provision. That the study be replicated in other counties/regions in Kenya reporting low circumcision rates and high HIV prevalence; and on health workers to establish their perceptions and attitudes on the involvement of female nurses in VMMC service provision in the country.
Key Words: Perceptions, Attitudes, VMMC, Non-Physician Clinicians, Female Nurses, Acceptability, Task Shifting/Task Sharing, Ambitious-time sensitive, Scale up.
INTRODUCTION
Female nurses in many countries in the continent including Kenya and by extension Homa Bay County are more in number compared to their male counterparts WHO/UNAIDS, (2007). Specifically, female nurses stand at 82% against 18% male nurses in Homa Bay County, (Wakaba et al., 2014). However, national policies are silent on the role of female nurses in the provision of voluntary medical male circumcision (VMMC) services National AIDS Control Council (2016). If the female nurses are fully accepted, they will certainly help in addressing the human resource needs for VMMC scale up National AIDS Control Council (2016). Therefore, this cross-sectional study was done in Rangwe Sub-County, Homa Bay County to gain knowledge on locals’ perceptions and attitudes on acceptability of female nurses in VMMC service provision.
Evidence from observational and meta-analytical studies and three randomized controlled trials conducted in Orange Farm in South Africa, Kisumu in Kenya, and Rakai District in Uganda between 2005 and 2007 demonstrated that male circumcision (MC) lowers the risk of Human Immunodeficiency virus (HIV) transmission and sexually transmitted infections (STIs) in heterosexual relationships by about 60%, (Auvert et al., 2005). Similarly, Westercamp and Bailey (2007) in a comprehensive review of studies on the acceptability of male circumcision (MC) among non-circumcising communities in sub-Saharan Africa state that on average, the proportion of men willing to be circumcised was 65%. Thus, the World Health Organization and The Joint United Nations Programme on HIV/AIDS (WHO/UNAIDS) recommended that countries and regions with low MC rates and high heterosexual HIV epidemics increase access to and availability of MC services as an efficacious HIV prevention intervention strategy for age groups at highest risk of acquiring HIV infection
The World Health Organization (WHO) estimates that on average, 30% of men aged 15 years and above are circumcised globally. However, some countries in East and Southern Africa still report low circumcision rates of below 20%. While countries still report low circumcision rates, approximately 36.7 million people are reported to be living with Human Immunodeficiency Virus and Acquired Immune Deficiency Syndrome (HIV/AIDS) worldwide WHO/UNAIDS, (2016).
Similarly, the Kenya AIDS Indicator Survey (KAIS) report shows MC rates of about 86% in men aged between 15-49 years in Kenya, with regional variations especially in parts of Nyanza Region where circumcision rates are still low, at about 51%. At the same time, on average, HIV prevalence among persons aged between 15-64 years is reported as 5.6% nationally, again with regional variation ranging from 15.1% in Nyanza to 2.1% in North Eastern. HIV prevalence among uncircumcised men aged 15-64 years is reported at 16.9% compared to 3.1% of circumcised men, (KAIS, 2012). Similarly, the Kenya County HIV Profile, (2016) reports MC rate of 52.6% and HIV prevalence of 26.7% in Homabay County. Thus, following the WHO/UNAIDS recommendations, 14 priority countries in East and Southern Africa including Kenya were identified to initiate programs to increase access to and availability of VMMC services. However, a study on VMMC scale up reveals that reliance on the few physicians has slowed down efforts to scale up VMMC programs in Kenya and other parts of the continent, Nyanga et al (2014). Similarly, a study by Ledikwe et al,2014 revealed that the ambitious, time-sensitive male circumcision targets required that large numbers of trained health care workers and other cadres of support personnel are in place. Therefore, Kenya, among other countries introduced “Task shifting” and “Task sharing” where non-physician clinicians including male and female were trained to provide of VMMC services. By the end of 2012, Kenya had implemented policies that allowed non-physician clinicians to provide VMMC services.
The Health Belief Model (HBM) as proposed by Rosenstock et al.1988 was used to explain behaviour of individuals as they engage in male circumcision activities (Figure 1). Basically, this model theorizes on people’s beliefs regarding the risk of a health problem and their perceptions on the benefits of taking actions to avoid it and analyses their readiness to take action. HBM directs individuals in decision-making which may result in either adopting a new behaviour or not in this case the acceptance of female nurses in performing MC especially where there are staffing challenges.
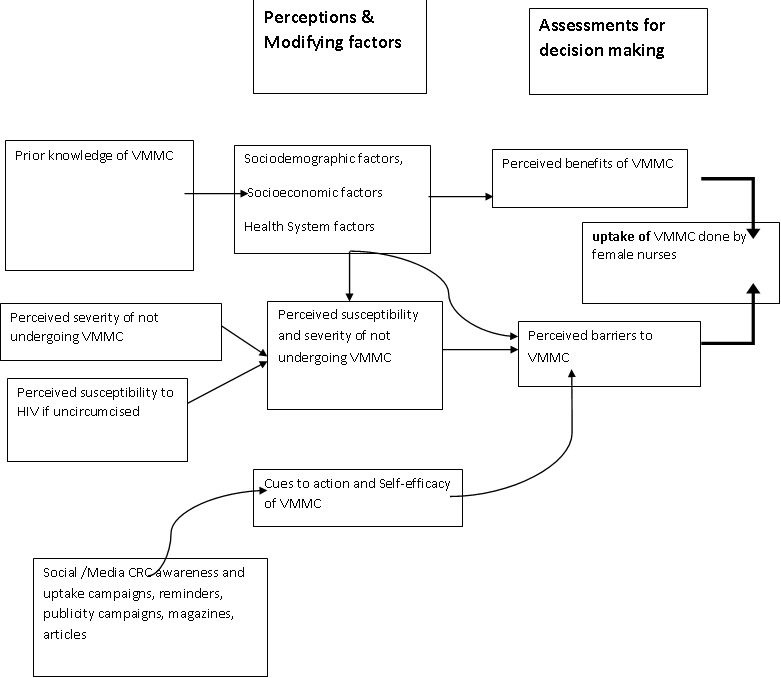
Figure 1 The Health Belief Model (Rosenstock et al.1988)
The objective was to establish locals’ perceptions and attitudes influencing acceptability of female nurses in VMMC service provision in Rangwe Sub-County, Homa Bay County. It aimed to address the following hypothesis: that men and their spouses are satisfied with MC performed by female nurses. It targeted males aged 18-50 years from one sub-county only. Additionally, the sensitivity of the topic could inhibit open discussions.
MATERIALS AND METHODS
This was a cross-sectional study that adopted both quantitative and qualitative approaches to data collection, analysis and presentation. This study was carried out in Rangwe Sub-County, Homa Bay County in May 2019. Some 384 circumcised and uncircumcised men aged between 18 and 50 years were recruited.
Study Design: A cross-sectional study in which both primary and secondary data were collected.
Study Location: Rangwe Sub-County, Homabay County in Nyanza Region
Sample Size calculation: A representative sample of 384 respondents was obtained from the target population of the 10,000 circumcised and uncircumcised men, aged 18-50 years in Rangwe Sub County using the Cochran formula
Subject Selection Method: Stratified Random Sampling, where stratification was done on eight health facilities. Thereafter random sampling was used where all circumcised and uncircumcised men between 18 – 50 years of age had equal chance of being selected.
Inclusion Criteria:
- Men aged between 18-50 years
- All were residents of the study area
- Participants who gave informed consent
Exclusion Criteria:
- The study excluded men who had conditions that could not allow them to make independent decisions
- The study excluded men who were visitors in the area at the time of the study
Procedure and Methods: Primary and secondary data were collected after obtaining the research consent, using both qualitative and quantitative data methods. The data collection process was undertaken in two weeks
Ethical Approval: Approval to carry out this study was sought and obtained from Great Lakes University, Kisumu. Clearance was obtained Great Lakes University, Kisumu Ethics and Research Committee. Research permit was obtained from the National Commission for Science, Technology and Innovation (NACOSTI). This permit was then presented to the relevant authorities in Homa Bay County Health Department, and the Hospital Administration at Rangwe Sub-County Hospital. Voluntary and informed consent of the respondents was sought after explaining the aim of the study.
Statistical Analyses: Statistical Packages for Social Science (SPSS) version 22 program was used are used at Confidence Level 0.05%. The barriers towards acceptance of female nurses in VMMC were determined by descriptive statistics and Chi-Square from the closed ended questionnaires and the qualitative information. Data was presented in the form of frequency tables and percentages. Qualitative data from open-ended questions were coded and included for analysis.
RESULTS
Demographic data is presented on Table 1 below. The results in indicate that the respondents were fairly distributed across the various age groups, with slightly more than half, 214 (55.7%) of the respondents aged between 18-32 years. The results also show that majority, 241 (62.8%) were married, 328 (85.4%) had 0-5 children, and 363 (94.5%) were Christians respectively. The results further indicate that only 135 (35.2%) of the respondents had post-secondary education, with a high proportion, 172 (44.8%) and 100 (26.0%) generating their income through farming and business respectively. A high proportion, 141 (36.7%) and 112 (29.2%) of the respondents were farmers and businessmen respectively.
Table 1: Demographic factors influencing acceptability of female nurses in VMMC service provision
| Demographic Characteristics | N=384 | Frequency | Percent | |
| Age distribution (years) | 18-22 | 384 | 76 | 19.8% |
| 23-27 | 77 | 20.1% | ||
| 28-32 | 61 | 15.9% | ||
| 33-37 | 60 | 15.6% | ||
| 38-42 | 53 | 13.8% | ||
| 43-47 | 34 | 8.9% | ||
| 48-50 | 23 | 6.0% | ||
| Marital status | Married | 384 | 241 | 62.8% |
| Unmarried | 124 | 32.3% | ||
| Widowed | 19 | 4.9% | ||
| Divorced | 0 | 0.0% | ||
| Level of Education | None | 384 | 15 | 3.9% |
| Primary | 104 | 27.1% | ||
| Secondary | 130 | 33.9% | ||
| Post-secondary | 135 | 35.2% | ||
| Number of children | 0-5 | 384 | 328 | 85.4% |
| 6-10 | 47 | 12.2% | ||
| 11-15 | 9 | 2.3% | ||
| No Response | 0 | 0.0% | ||
| Religion | None | 384 | 4 | 1.0% |
| Christian | 363 | 94.5% | ||
| Islam | 11 | 2.9% | ||
| Hinduism | 1 | 0.3% | ||
| Traditional African | 4 | 1.0% | ||
| Atheist | 1 | 0.3% | ||
| Source of Income | None | 384 | 46 | 12.0% |
| Formal employment | 66 | 17.2% | ||
| Farming | 172 | 44.8% | ||
| Business | 100 | 26.0% | ||
| Occupation | None | 384 | 42 | 10.9% |
| Businessman | 112 | 29.2% | ||
| Farmer | 141 | 36.7% | ||
| Health Worker | 42 | 10.9% | ||
| Teaching | 47 | 12.2% | ||
Table 2 below shows results on Locals’ Perceptions and Attitudes on VMMC by female nurses. Specifically, these results indicate that majority, 303 (78.9%) of the respondents were of the opinion that VMMC was freely discussed at their place of work or in the community. A further 200 (65.1%) of the respondents were of the opinion that their workmates and the community respect individual’s choice with regard to VMMC, while 70 (22.8%) indicated that uncircumcised individuals are ridiculed/stigmatized and 30 (9.8%) indicated that circumcised individuals are ridiculed/stigmatized. Another 7 (2.3%) of the respondents indicated that their workmates or the community do not want to hear about VMMC. The results further indicate that, of the respondents who were circumcised by female nurses, majority, 95 (88.0%) were comfortable being circumcised by a female nurse, with 91 (84.3%) indicating that they were very satisfied with the circumcision by the female nurse.
Majority, 86 (81.9%) of the respondents who were circumcised by female nurses and were married indicated that their partners were satisfied that they were circumcised by a female nurse.
Table 2: Locals’ perceptions and attitudes on VMMC by female nurses.
| Perceptions and attitudes on VMMC | N=384 | Frequency | Percent | |
| VMMC freely discussed in workplace and in the community | Yes | 384 | 303 | 78.9% |
| No | 81 | 21.1% | ||
|
Attitude about VMMC |
Circumcised community ridiculed | 307 | 30 | 9.8% |
| Uncircumcised community ridiculed | 70 | 22.8% | ||
| Individual’s choice respected | 200 | 65.1% | ||
| Do not want to hear | 7 | 2.3% | ||
| Comfortable being circumcised by female nurse | Yes | 108 | 95 | 88.0% |
| No | 13 | 12.0% | ||
| SWMC by female nurse | Very satisfied | 108 | 91 | 84.3% |
| Somewhat satisfied | 12 | 11.1% | ||
| Very dissatisfied | 3 | 2.8% | ||
| Somewhat dissatisfied | 2 | 1.9% | ||
| Partner is satisfied with MC by FN | Yes | 105 | 86 | 81.9% |
| No | 19 | 18.1% | ||
In order to identify the locals’ perceptions and attitudes influencing acceptability of female nurses in VMMC service provision, the study conducted the chi-square test of association at the level of significance of alpha=0.05.
This test revealed that MC, when freely discussed at the work place or in the community had a statistically significant association with acceptability of female nurses in the provision of VMMC services (p = 0.000). This therefore, shows that a significant majority (89%) of the respondents whose places of work or community freely discussed MC, compared to 57% of the respondents whose places of work or community did not freely discuss MC, would recommend that female nurses be trained on VMMC, and be allowed to provide the VMMC services.
However, the attitude of the respondents’ workmates or community had no statistically significant association with acceptability of female nurses in the provision of VMMC services (p = 0.054). In other words, there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents whose places of work or community freely discussed MC and those whose places of work or community did not freely discuss MC.
The results further indicate that the respondents’ comfortableness with the idea of being circumcised by a female nurse had a statistically significant association with acceptability of female nurses in the provision of VMMC services, (p = 0.000). This shows that a significant majority (94%) of the respondents who were comfortable being circumcised by a female nurse, compared to only 38% of the respondents who were not comfortable, would recommend that female nurses be trained on MMC, and be allowed to provide the VMMC services. These results are shown in Table 3 below.
Table 3: Relationship between Locals’ Perceptions/attitudes and VMMC acceptability by female nurses
| Accept VMMC by female nurse | |||||||
| N | Yes | No | X2 | df | p | ||
| VMMC freely discussed in the community | Yes | 384 | 269 (89%) | 34 (11%) | 44.370a | 1 | 0.000 |
| No | 46 (57%) | 35 (43%) | |||||
| Attitude about VMMC | Circumcised ridiculed | 307 | 27 (90%) | 3 (10%) | 7.661a | 3 | 0.054 |
| Uncircumcised ridiculed | 64 (91%) | 6 (9%) | |||||
| Individual’s choice respected | 178 (89%) | 22 (11%) | |||||
| Do not want to hear | 4 (57%) | 3 (43%) | |||||
| Comfortable being circumcised by female nurse | Yes | 108 | 89 (94%) | 6 (6%) | 30.908a | 1 | 0.000 |
| No | 5 (38%) | 8 (62%) | |||||
| SWMC by female nurse | Very satisfied | 108 | 87 (96%) | 4 (4%) | 42.346a | 3 | 0.000 |
| Somewhat satisfied | 5 (42%) | 7 (58%) | |||||
| Very dissatisfied | 2 (67%) | 1 (33%) | |||||
| Somewhat dissatisfied | 0 (0%) | 2 (100%) | |||||
| Partner is satisfied with MC by FN | Yes | 105 | 82 (95%) | 4 (5%) | 31.003a | 1 | 0.000 |
| No | 9 (47%) | 10 (53%) | |||||
DISCUSSION
This is one among the few studies that focused on the acceptability of Female Nurses in the provision of voluntary medical male circumcision (VMMC) services. Darby et al. (2003) states that male circumcision is one of the oldest and most common surgical procedures practiced worldwide performed by trained doctors, nurses and clinical officers, and traditional circumcisers in some communities. However, it did not specifically dwell on acceptability of circumcisers based on their gender.
Therefore, this study sought to establish the level of acceptability of female nurses in the provision of voluntary medical male circumcision services in Rangwe Constituency, Homa Bay County. The level of acceptability was assessed by asking the respondents to indicate whether they would personally accept VMMC by a female nurse, whether they would encourage VMMC by a trained female nurse and whether they would recommend that female nurses be trained and be allowed to offer VMMC services.
Descriptive analysis (frequencies and percentages) and inferential analysis (Chi-Square test) was used to determine the relationship between acceptability of female nurses in the provision of VMMC services (dependent variable); and demographic factors, locals’ perceptions and attitudes and social/cultural factors (independent variables).
In order to assess the locals’ perceptions and attitudes, respondents were asked to indicate whether MC is freely discussed at their place of work or in the community and also give their opinion on the general attitude of their work mates or the community about MC. The respondents who were circumcised by a female nurse were also asked to indicate whether they were comfortable being circumcised by a female nurse, indicate the level of their satisfaction with the services of the female nurse and whether their partners were satisfied that they were circumcised by a female nurse.
The study determined that majority, 303 (78.9%) of the respondents were of the opinion that MC was freely discussed at their place of work or in the community. Additionally, 200 (65.1%) of the respondents were of the opinion that their workmates or the community respect individual’s choice with regard to MC, while 70 (22.8%) indicated that uncircumcised individuals are ridiculed/stigmatized and 30 (9.8%) indicated that circumcised individuals are ridiculed/stigmatized.
Another 7 (2.3%) of the respondents indicated that their workmates or the community do not want to hear about MC. The results further indicate that, of the respondents who were circumcised by female nurses, majority, 95 (88.0%) were comfortable being circumcised by a female nurse, with 91 (84.3%) indicating that they were very satisfied with the circumcision by the female nurse.
Majority, 86 (81.9%) of the respondents who were circumcised by female nurses and were married indicated that their partners were satisfied that they were circumcised by a female nurse. As stated above, the study conducted the chi-square test of association at the level of significance of alpha=0.05 in order to identify the locals’ perceptions and attitudes influencing acceptability of female nurses in VMMC service provision
This revealed that MC when freely discussed at the work place or in the community has a statistically significant association with acceptability of female nurses in the provision of VMMC services (p = 0.000). This therefore, shows that a significant majority (89%) of the respondents whose places of work or community freely discussed MC, compared to 57% of the respondents whose places of work or community did not freely discuss MC, would recommend that female nurses be trained on VMMC, and be allowed to provide the VMMC services.
However, the attitude of the respondents’ workmates or community had no statistically significant association with acceptability of female nurses in the provision of VMMC services (p = 0.054). In other words, there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents whose places of work or community freely discussed MC and those whose places of work or community did not freely discuss MC.
The results also indicate that the respondents’ comfortableness with the idea of being circumcised by a female nurse had a statistically significant association with acceptability of female nurses in the provision of VMMC services, (p = 0.000). This shows that a significant majority (94%) of the respondents who were comfortable being circumcised by a female nurse, compared to only 38% of the respondents who were not comfortable, would recommend that female nurses be trained on MMC, and be allowed to provide the VMMC services.
In other words, there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents who were comfortable being circumcised by a female nurse and those who were not comfortable. The results further indicate that the respondents’ level of satisfaction with the circumcision by a female nurse had a statistically significant association with acceptability of female nurses in the provision of VMMC services, (p = 0.000).
Similarly, this shows that a significant majority (96%) of the respondents were very satisfied being circumcised by a female nurse, compared to 42% who were somehow satisfied and 67% who were very dissatisfied, even though, they would recommend that female nurses be trained on VMMC, and be allowed to provide the VMMC services. In other words, there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents who were very satisfied being circumcised by a female nurse, and those who were somehow satisfied or very dissatisfied.
Additionally, results indicate that a partner’s satisfaction with her spouses’ circumcision by a female nurse had a statistically significant association with acceptability of female nurses in the provision of VMMC services (p = 0.000). This shows that a significant majority (95%) of the respondents whose partners were satisfied with their circumcision by a female nurse, compared to 47% who were not satisfied, would recommend that female nurses be trained on VMMC, and be allowed to provide the VMMC services.
In other words, there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents whose partners were satisfied with their circumcision by a female nurse and those whose partners were not satisfied. Overall, this result is supported by a study by Milly (2009) which states that some men would not mind circumcision by female nurses arguing that they are good medics, and that they perform the procedure with precision.
CONCLUSION
The study revealed evidence on acceptability of female nurses as providers of VMMC services in Homa Bay County. However, acceptability was subject to free VMMC discussions at the work place or in the community; comfortableness and satisfaction with circumcision by a female nurse, and partners’ satisfaction with the circumcision of the spouse by a female nurse influence acceptability of female nurses in the provision of VMMC services.
This study also revealed that there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents who were comfortable being circumcised by a female nurse and those who were not comfortable. The results further indicate that the respondents’ level of satisfaction with the circumcision by a female nurse had a statistically significant association with acceptability of female nurses in the provision of VMMC services, (p = 0.000).
Similarly, this shows that a significant majority (96%) of the respondents were very satisfied being circumcised by a female nurse, compared to 42% who were somehow satisfied and 67% who were very dissatisfied, even though, they would recommend that female nurses be trained on VMMC, and be allowed to provide the VMMC services. In other words, there is a significant difference in acceptability of female nurses in the provision of VMMC services between respondents who were very satisfied being circumcised by a female nurse, and those who were somehow satisfied or very dissatisfied.
Additionally, results indicate that a partner’s satisfaction with her spouses’ circumcision by a female nurse had a statistically significant association with acceptability of female nurses in the provision of VMMC services (p = 0.000). This shows that a significant majority (95%) of the respondents whose partners were satisfied with their circumcision by a female nurse, compared to 47% who were not satisfied, would recommend that female nurses be trained on VMMC, and be allowed to provide the VMMC services.
RECOMMENDATIONS FROM THE STUDY
a) That the county government of Homa Bay develops appropriately tailored messages for communities to use as they engage in free discussions on VMMC by female nurse at workplaces and in the community;
b) That sensitization programmes on VMMC service provision by female nurses involve both men and their partners given that the perceptions and attitudes of both tend to influence acceptability of female nurses in VMMC service provision;
c) That the county government actively engages and or consults communities to help with decision making on policy change regarding the involvement of female nurses in VMMC service provision.
Additionally, this study should be replicated in other counties/regions in Kenya that still report low circumcision rates and high HIV prevalence. This will help generate more knowledge that would inform policy formulation and strategic planning on MC strategies in the country. Another area should be a study on health workers in general to establish their perceptions and attitudes on the involvement of female nurses in VMMC service provision in the country.
REFERENCES
- Auvert B; Bailey R.C; Lagarde E; Sobngwi-Tamekou J; Westercamp et al (2005). Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk in Orange Farm, South Africa; Kisumu in Kenya, and Rakai in Uganda: the ANRS 1265 Trial. PLoS Med.(PubMed)
- Fishbein and Aizen, (1970, 1980). The Theory of Reasoned Action Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, et al., (2007). Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet. 2007;369:657–666. {PubMed}
- Ledikwe, Seema, Nyanga, et al, (2014). Voluntary medical male circumcision for HIV prevention: Review on monetary investment
- Mavhu, W., Frade, S., Yongho, A. M., Farrell, M., Hatzold, K., et al (2014). Provider attitudes towards voluntary medical male circumcision scale-up in Kenya, South Africa, Tanzania and Zimbabwe. PloS One, 9(5), e82911.
- Milly, (2009). Should female nurses be allowed to circumcise men?. A male circumcision study in Zimbabwe
- Mwijarubi, M. (2015). Medical male circumcision services predominantly rely on a female nursing workforce: A Review on Provider Attitudes on male circumcision.
- National AIDS and STI Control Programme in Tanzania, (2013). Kenya AIDS Indicator Survey: Final Report
- National AIDS Control Council (2016). Kenya County HIV Profiles.
- Nyanga, and Ledikwe (2014). Maximizing utilization of health workforce for VMMC scale up
- Nyanga and Ledikwe, (2014). Reliance on the few physicians has slowed down efforts to scale up VMMC programs in Kenya and other parts of the continent. a Cohort Study on VMMC scale up reveals in East and Southern Africa
- Rosenstock, (1984). Health Belief Model: Modified version
- Umar, E., Mandalazi, P., Jere, D., (2013). Should female health providers be involved in medical male circumcision? Narratives of newly circumcised men in Malawi. Malawi Med J- Sep.2013.25(3):72-77
- Wakaba, M., Mbindyo, P., Ochieng, J., Kiriinya, R.., Waudo, A., et al (2014). The Public Sector Nursing Workforce in Kenya: A county-level analysis. Human Resources for Health, 12, 6.
- WHO/UNAIDS, (2007). Male circumcision: global trends and determinants of prevalence, safety and acceptability. AWHO Publication
- WHO/UNAIDS, (2016). Voluntary medical male circumcision for HIV prevention in 14 priority countries in East and Southern Africa: A Progress Report. A WHO Publication
- https://www.standardmedia.co.ke/business/article/1144019176. Are you Safer facing the Knife by a man or woman?: Assessing Voluntary medical male circumcision scale up strategies in Kenya, Otieno K., (2009)