
Healthy Learning Environments, Stress Management and Mental Health in Higher Education Students
- Tania Gaspar
- Susana Pestana
- Sofia Sousa
- Marta Barata
- Nuno Loureiro
- 266-274
- Mar 27, 2025
- Public Health
Healthy Learning Environments, Stress Management and Mental Health in Higher Education Students
Tania Gaspar1*, Susana Pestana2, Sofia Sousa1, Marta Barata1 and Nuno Loureiro2
1Lusofona University/Hei-Lab; Aventura Social Association
2Polytechnic Institute of Beja
DOI: https://doi.org/10.51244/IJRSI.2025.121500026P
Received: 18 February 2025; Accepted: 22 February 2025; Published: 27 March 2025
ABSTRACT
Educational institutions contribute to the well-being, health and performance of students. The aim of this study is to assess the mental health and well-being needs of higher education students by studying the healthy learning environment and its relationship with students’ mental health, and to understand the role of stress management skills in promoting mental health and healthier adjustment. The study used the Ecosystems of Healthy Learning Environments (EA2S) instrument and involved 521 students, 359 (69.4 %) of whom were female. Regarding the age of the students, 26.2 % were aged up to 19 (n=127), 64.3 % between 20 and 30 (n=311), 4.1 % between 31 and 40 (n=20) and 5.4 % 41 or over (n=26). The EA2S instrument consists of a total of 62 items organized into 9 dimensions. A moderation mediation model was carried out in order to understand the relationship between a healthy learning environment and students’ mental health and the mediating role of stress management skills in this relationship. We found that there is a relationship between a healthy learning environment and students’ mental health, and that this relationship is effectively mediated by stress management skills. The study refers to a multidomain intervention with the aim of promoting psychological health, well-being and skills, academic engagement and preventing higher education students from dropping out of school, through the development of psychological intervention, prevention and health promotion activities and training based on scientific evidence.
Keywords: ecosystems; higher education; wellness; stressors; health
INTRODUCTION
Mental health represents a state of well-being that enables a person to cope with the normal stresses of life, realize their abilities, learn well, work well and contribute to their community[1]. As an essential component of health and well-being, it underpins our individual and collective abilities to make decisions, establish interpersonal relationships and shape the world we live in. However, throughout our lives here are various factors (individual, social, and structural) that, in combination, can prove to be protective or have a less positive influence on our mental health, making us more vulnerable to possible mental health problems. A recent study published by the OECD/European Union[2] points to revealing results, in that in addition to the direct impact that the COVID-19 pandemic has had on health, other factors such as fear, uncertainty, prolonged periods of social isolation and interruptions in education and employment have seriously disrupted the lives and routines of young people. It has exacerbated many of the risk factors associated with poorer mental health and weakened many of the protective factors, leading to an unprecedented increase in mental health problems, especially among the younger population. The expansion of Higher Education (HE) can be understood not only by the larger number of students[3,4], but also by its diversity in terms of heterogeneity, namely different social and cultural backgrounds, as well as different educational experiences and expectations[4,5], which translates into a series of demands in terms of the transition process[5]. This transition can be characterized by a series of changes that occur in terms of the new demands arising from the role assumed as a student or the learning environment[6]. It represents a significant change in the student’s life, self-perception and learning, namely towards new meanings of understanding, development and maturity[4]. This transition process not only involves a change in study-related activities and the demands of time management[5,7,8], but it also involves a new social situation such as stress related to the financial situation, making new friends[5], moving away from home[4-6,9] or becoming an independent adult[4]. Higher education students are expected to work independently, but many have difficulty adjusting to teaching methods, meeting deadlines or understanding the best approach to learning[7], as well as poor self-regulation skills to study in a way that is considered effective[8,10]. Considering the demands related to the new role assumed and the new learning environment, this transition can be stressful[3,11,12], and students often question their philosophy of commitment and permanence in this academic path, which has consequences for their long-term functioning[13]. Several studies have identified a high prevalence of mental health problems among higher education students, which is often associated with the challenges experienced not only in terms of the transition to this cycle of education, but also throughout the academic journey, such as the change of residence, the high workload, the academic demands and pressures or the need to reconcile academic life with professional life[13-16]. If before the COVID-19 pandemic, the burden related to mental health problems was already quite significant among the younger European population, namely symptoms of depression and anxiety, as well as suicidal ideation[2]. The results point to an increase in these problems in the pandemic and post-pandemic period[2,12,17]. Diverse studies[12,18,19] show that during and after the pandemic, higher education students had high levels of anxiety, depression and emotional problems. As stated in the Programme for the Promotion of Mental Health in HE[20], the mental health and well-being of HE students is essential for them to develop and achieve success in their academic career and in their training process and overall personal development. Considering that around 446,000 students are currently enrolled in HE (university and polytechnic education)[21], the majority of whom are between the ages of 18 and 25 (ages that experts identify as critical for the onset of serious mental illness) and that the transition to HE is experienced by many students with difficulties in adapting, adjusting, manifestations of anxiety or other symptoms that impact on their mental health. So, it is imperative to create and implement differentiated responses in the area of mental health and well-being. Considering the importance that higher education assumes in students’ lives, it is important to recognize that for an adequate transition and effective integration into the academic context, it is essential that they know, anticipate and reflect on a set of new challenges in this new stage of their lives and that they know the context, strategies and support structures available to them[22].
This study, carried out at a Higher Education Institution in Alentejo (south of the country) in 2023, aims to assess the mental health and well-being needs of students from the different training programmes by studying the healthy learning environment and its relationship with students’ mental health, and to understand the role of stress management skills in promoting mental health and healthier adjustment.
MATERIALS AND METHODS
Participants
The study involved a total of 521 students, 359 (69.4%) female and 158 (30.6%) male. Regarding the age of the students, 26.2 % were aged up to 19 (n=127), 64.3 % between 20 and 30 (n=311), 4.1 % between 31 and 40 (n=20) and 5.4 % aged 41 or over (n=26). 7.9 % of students reported having children (n=41). 25.3% of students currently live in city alone (n=132), 31.3% with 1 or 2 people (n=163), 38% with 3 or 4 people (n=198) and 5.4% with 5 or more people (n=28). With regard to schooling, 17.5% of students have already completed a Higher Technical Course (n=91), 19.5% a Professional Course (n=101), 14.1% a Degree (n=73), 1.3% a Postgraduate Course (n=7), 1.3% a Master’s Degree (n=7) and 25.6% have not yet completed any of the above (n=133). 13.8 % of students are currently studying a Higher Technical Course (n=67), 2.3 % a Professional Course (n=11), 73.6 % a Bachelor’s Degree (n=356) and 9.1 % a Master’s Degree (n=44). Regarding the year in which they were enrolled, 53.2 % of students were enrolled in the 1st year (n=234), 25.2 % in the 2nd year (n=111), 16.4 % in the 3rd year (n=72) and 5.2 % in the 4th year (n=23).
Instruments
The Ecosystems of Healthy Learning Environments (EA2S) instrument[23] consists of a total of 62 items organised into 9 dimensions based on the Healthy Workplaces model proposed by the World Health Organization[24]. The Ethics and Ecosystems Values dimension has 8 items, Commitment to Leadership has 6 items, Student Involvement has 7 items, Psychosocial Risks related to content and relationships with leadership has 12 items, Psychosocial Risks related to Well-being and Mental Health has 5 items, Physical Environment has 5 items, Distance Learning has 3 items, Community Involvement has 12 items and Resources for Personal Health has 4 items. All questions have a 5-point Likert response scale. The instrument revealed adequate internal consistency for all dimensions (range between α =.84 and α =.93).
The DASS (Depression, Anxiety and Stress Scale)[25,26] consists of 21 items and is organized into three dimensions: stress, depression and anxiety, each with 7 items respectively. The higher the score, the higher the level of stress, depression and anxiety. The Total score of the scale was used for this study. All questions have a 4-point Likert-type scale where 1 represents Not applied to me at all and 4 represents Applied to me most of the time. The instrument revealed adequate internal consistency for all dimensions (range between α =.81 and α =.88).
The 4-item version of the Stress Perception Scale (EPS) was used to assess the degree to which an individual evaluates their life situations as stressful and their stress management skills[27,28] which in the present study revealed adequate internal consistency (α =.77). All questions have a 5-point Likert-type scale where 1 represents strongly disagree and 5 represents strongly agree. A higher score obtained in the scale reveals a less positive perception of stress management.
Procedure
The instrument was submitted to and approved by the Ethics Committee of the Prof Fernando Fonseca Hospital, reference EPE 031/2021. The sample was obtained by convenience. Higher education institutions that agreed to participate received the instrument via a link and disseminated the link internally to their students. The link gave access to an explanation of the study, contact details for the researchers to clarify any doubts, information on confidentiality, anonymity and the voluntary nature of participation. The participant only had access to the instrument after signing the informed consent form.
RESULTS
Regarding education, 16.3% of participants had a professional course or a higher technical course (n=78), and 83.7% had a bachelor’s or master’s degree (n=400). 21.1% were student workers (n=110) and 78.9% were full-time students (n=411). 72.6% of participants were displaced students (n=378) and 27.4% were non-displaced students (already living in the area of the higher education institution) (n=143).
Values related to mental health (Depression, Anxiety and Stress) and stress management skills are moderate. The perception of a healthy learning environment is high (Table 1).
Table 1. Descriptive statistics
| Min. | Max. | M | SD | |
| Depression Anxiety and Stress Scale (DASS) | 21.00 | 84.00 | 36.81 | 13.41 |
| Perceived Stress Scale | 4.00 | 20.00 | 11.48 | 2.74 |
| Healthy Learning Environment (EA2S) | 39.00 | 112.00 | 78.61 | 11.34 |
The correlations between the scales are statistically significant, indicating the presence of a moderate positive correlation between the Depression Anxiety and Stress Scale and the Perceived Stress Scale (r=0.621), and a moderate negative correlation between the Depression, Anxiety, and Stress Scale and the perception of a healthy learning environment (r=-0.440), as well as between the Perceived Stress Scale and the perception of a healthy learning environment (r=-0.427) (Table 2).
Table 2. Correlations between scales
| Depression Anxiety and Stress Scale (DASS) | Perceived Stress Scale (Cohen) | Healthy Learning Environment (EA2S) | |
| Depression Anxiety and Stress Scale (DASS) | 0.621*** | -0.440*** | |
| Perceived Stress Scale | -0.427*** | ||
| Healthy Learning Environment (EA2S) |
*** p<0.001
With regard to sex differences, according to Table 3, the values obtained in the Depression Anxiety and Stress Scale by female students (M = 37.92; SD = 13.46; n = 359) were higher than those of male students (M = 33.97; SD =12.60; n = 158), and this difference was statistically significant (t (515) = 3.127; p = 0.002, d=0.30). Similarly, the values obtained in the Stress Perception Scale by female students (M = 11.78; SD = 2.54; n = 359) were higher than those of male students (M = 10.74; SD = 3.01; n = 158), and this difference was statistically significant (t (259.33) = 3.794; p = <0.001; d = 0.39). Regarding the perception of a healthy learning environment, no statistically significant differences were found between groups.
Table 3. Comparison between groups in terms of gender
| Female
(n=359) |
Male
(n=158) |
t/sig | |||
| M | SD | M | SD | ||
| Depression Anxiety and Stress Scale (DASS) | 37.92 | 13.46 | 33.97 | 12.60 | 3.127** |
| Perceived Stress Scale | 11.78 | 2.54 | 10.74 | 3.01 | 3.794*** |
| Healthy Learning Environment (EA2S) | 78.16 | 11.25 | 79.89 | 11.34 | -1.601 |
** p<0.01; *** p<0.001
With regard to education level, according to Table 4, the perception of a healthy learning environment among students with a professional course or a higher technical course (M = 80.88; SD = 11.02; n = 78) was higher than that of students with a bachelor’s or master’s degree (M = 77.99; SD = 11.48; n = 400), and this difference was statistically significant (t (476) = 2.052; p = 0.041, d = 0.25). No statistically significant differences were found between groups in relation to the Depression Anxiety and Stress Scale and the Perceived Stress Scale.
Table 4. Comparison between groups regarding education
| Professional course or higher technical course (n=78) | Bachelor’s or master’s degree
(n=400) |
t/sig | |||
| M | SD | M | SD | ||
| Depression Anxiety and Stress Scale (DASS) | 36.58 | 13.92 | 36.94 | 13.22 | -0.221 |
| Perceived Stress Scale | 11.31 | 2.49 | 11.52 | 2.80 | -0.615 |
| Healthy Learning Environment (EA2S) | 80.88 | 11.02 | 77.99 | 11.48 | 2.052* |
* p<0.05
With regard to the student status, according to Table 5, the perception of a healthy learning environment among participants who are working students (M = 80.52; SD = 11.05; n = 110) was higher than that of participants who are full-time students (M = 78.09; SD = 11.38; n = 411), and this difference was statistically significant (t (519) = 1.995; p = 0.047; d = 0.21). Regarding the Depression Anxiety and Stress Scale, and the Perceived Stress Scale, no statistically significant differences were found between groups.
Table 5. Comparison between groups regarding student status
| Working student (n=110) | Full-time student
(n=411) |
t/sig | |||
| M | SD | M | SD | ||
| Depression Anxiety and Stress Scale (DASS) | 35.61 | 14.38 | 37.13 | 13.14 | -1.056 |
| Perceived Stress Scale | 11.35 | 2.71 | 11.51 | 2.75 | -0.570 |
| Healthy Learning Environment (EA2S) | 80.52 | 11.05 | 78.09 | 11.38 | 1.995* |
* p<0.05
With the aim of examining a potential mediating effect of stress perception in the predictive relationship between the learning environment and mental health, a mediation model was developed (Figure 1). The results indicate that in the tested mediation model, the assessed indirect effect is significant, with stress perception acting as a mediating factor in the relationship between a healthy learning environment and mental health (b = -0.23; SE = 0.02; IC 95% = [-0.27; -0.18]). The model explains 42% of the variation. Thus, it is observed that the presence of a healthy learning ecosystem influences students’ mental health, and the promotion of stress management skills can serve as a protective factor for mental health and the promotion of stress management skills can serve as a protective factor for mental health in this context.
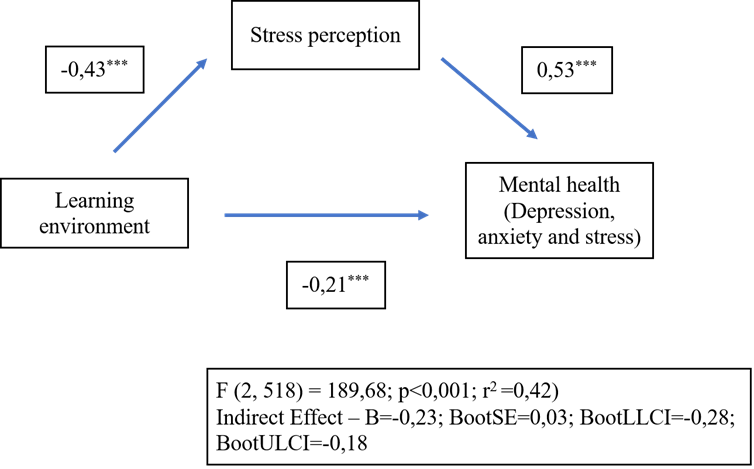
*** p<0.001
Figure 1. Mediation model
DISCUSSION
This study aims to deepen our understanding of healthy learning ecosystems, how they relate to students’ mental health and what role the perception of stress management skills plays in promoting the mental health of higher education students.
We found that students have a positive and healthy perception of the learning environment. This ecosystem includes the organizational culture, interpersonal relationships with colleagues, teachers, and other higher education staff, and the psychosocial environment related to involvement and appreciation. For students, the higher education institution is a positive and healthy place to learn and socialize.
With regard to mental health, related to symptoms of stress, anxiety and depression, we found that the students were at moderate risk. In terms of perceived stress management skills, we also found moderate values.
When we compare boys and girls, we see that girls report worse indicators of mental health and stress management skills when compared to boys. These results are consistent with recent studies confirming that girls show less positive mental health indicators [2,12,14,15,17].
Comparing students according to their level of education and professional status, we see that it is undergraduate students and working students who show a more positive perception of the healthy learning ecosystem when compared to postgraduate students and students who do not carry out any professional activity respectively.
The high prevalence of mental health problems among higher education students is often associated with the challenges that this population faces throughout their academic career, such as having to move house, the workload, academic demands and pressure, or having to reconcile academic and professional life [13-16]. The presence of mental health problems has an high impact on the way students fulfils their social role and on their academic performance. In some cases, it can lead to dropping out of higher education and consequences for the individual’s long-term functioning [13]. In a study by Mofatteh[16], various risk factors associated with stress, anxiety and depression in higher education students were identified, such as psychological factors (e.g. low self-esteem, self-confidence, personality types and loneliness), academic factors (e.g., field of study, completion of studies and uncertainty about the future, high workload, academic pressure, low academic performance, exam/assessment periods), biological factors (e.g. physical health problems and chronic illness, female gender), lifestyle factors (e.g., consumption of alcohol, tobacco and other illicit substances, unhealthy eating habits, lack of exercise/physical activity and insufficient quantity and quality of sleep), social factors (e.g. lack of social support and family support, non-involvement in social events/activities (e.g., clubs and academic groups or sports teams), sexual victimization, excessive use of the internet and social networks, belonging to ethical and religious minority groups, stigma associated with mental health) and economic factors (e.g. lack of financial support, low family income, childhood poverty) [14,15,29-31].
A mediation model was carried out with the aim of understanding the relationship between a healthy learning environment and students’ mental health and the mediating role of stress management skills in this relationship. We found that there is a relationship between a healthy learning environment and students’ mental health, and that this relationship is effectively mediated by stress management skills.
This result emphasizes the important role that higher education institutions play in promoting and protecting students’ mental health, and that the promotion and development of stress management skills related to managing challenging and new situations and confidence in the ability to manage and deal with problems are fundamental to better mental health among higher education students.
One of the protective factors for mental health identified in the literature is the acquisition of personal and social competences by students, with a view to greater adaptability and problem-solving skills. These skills are associated with academic performance and school success, as well as young people’s social and emotional well-being[32]. Thus, Higher Education Institutions (HEIs), as organizations that promote healthy development, play an important role in promoting skills, well-being and mental health among students, teachers and non-teaching staff. HEI intervention in the area of mental health was initially focused on solving individual mental health problems, but this perspective has been evolving, providing broader actions and services that consider the individual as a whole, in interaction with others and the context[16,33,34].
This integrative and comprehensive perspective, which is the one we adopt, argues that interventions in organizations, particularly in HEIs, should be global, preventive and promote good individual, collective and organizational functioning, with a view to contributing to the well-being of all those involved [14,15,19]. In addition to the aspects already mentioned, studies show that interventions that are integrated into day-to-day practice and are present in the culture of the organization, seeking to involve all stakeholders in the context, namely students, teachers and non-teaching staff, as well as networking with external entities and partners, contribute to better development of young people’s social and emotional skills[32,35,36].
We conclude that students’ positive development and learning are closely related to their mental health and subjective well-being. The university ecosystem, as a context that promotes development, can act as a risk context for psychopathology, but it can also be a privileged promoter of psychological health, well-being, academic and professional success.
A multidomain intervention is advocated with the aim of promoting psychological health, well-being and skills, academic engagement and preventing higher education students from dropping out of school, through the development of psychological intervention, prevention and health promotion activities and training based on scientific evidence.
“The authors declare no conflict of interest.”
REFERENCES
- World Health Organization. Mental health: strengthening our response; 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
- OECD/European Union. Health at a Glance: State of health in the EU cycle. OECD Publishing; 2022. https://doi.org/10.1787/507433b0-en
- Gill AJG. Difficulties and support in the transition to higher education for non-traditional students. Research in Post-Compulsory Education 2021; 26(4): 410-441. https://doi.org/10.1080/13596748.2021.1980661
- Hussey T, Smith P. Transitions in higher education. Innovations in Education and Teaching International 2010; 47(2): 155-164. https://doi.org/10.1080/14703291003718893
- Hultberg J, Plos K, Hendry GD, et al. Risk factors associated with stress, anxiety, and depression among university undergraduate students. Journal of Further and Higher Education 2008; 32(1): 47-57. https://doi.org/10.1080/03098770701781440
- Coertjens L, Brahm T, Trautwein C, et al. Students’ transition into higher education from an international perspective. Higher Education 2017; 73: 357-369. https://doi.org/10.1007/s10734-016-0092-y
- Brooman S, Darwent S. Measuring the beginning: A quantitative study of the transition to higher education. Studies in Higher Education 2014; 39(9): 1523-1541. https://doi.org/10.1080/03075079.2013.801428
- Perander K, Londen M, Holm G. Supporting students’ transition to higher education. Journal of Applied Research in Higher Education 2020; 3(2): 622-632. https://doi.org/10.1108/jarhe-01-2020-0005
- Arnett JJ. College students as emerging adults: The developmental implications of the college context. Emerging Adulthood 2016; 4(3): 219-222. https://doi.org/10.1177/2167696815587422
- Pintrich PR, Zusho A. The development of academic self-regulation: The role of cognitive and motivational factors. In: Development of achievement motivation. Academic Press; 2002. pp. 249-284. https://doi.org/10.1016/b978-012750053-9/50012-7
- McSweeney F. ‘Moving In’: Difficulties and support in the transition to higher education for in-service social care students. Social Work Education 2014; 33(3): 317-337. https://doi.org/10.1080/02615479.2013.770832
- Wu T, Jia X, Shi H, et al. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. Journal of Affective Disorders 2021; 281: 91-98. https://doi.org/10.1016/j.jad.2020.11.117
- Ebert DD, Mortier P, Kaehlke F, et al. Barriers of mental health treatment utilization among first‐year college students: First cross‐national results from the WHO World Mental Health International College Student Initiative. International journal of methods in psychiatric research 2019; 28(2): e1782. https://doi.org/10.1002/mpr.1782
- Gaspar T, Gomez-Baya D, Guedes FB, et al. Health management: Evaluating the relationship between organizational factors, psychosocial risks at work, performance management, and hospital outcomes. Healthcare 2023; 11(20): 2744. https://doi.org/10.3390/healthcare11202744
- Gaspar T, Telo E, Rocha-Nogueira J, et al. Manual de Boas Práticas: Promoção de Ambientes de Trabalho Saudáveis. Laboratório Português de Ambientes de Trabalho Saudáveis; 2023.
- Mofatteh M. Risk factors associated with stress, anxiety, and depression among university undergraduate students. AIMS Public Health 2021; 8(1): 36-65. https://doi.org/10.3934/publichealth.2021004
- Wei C, Ma Y, Ye JH, et al. First-year college students’ mental health in the post-COVID-19 era in Guangxi, China: A study demands-resources model perspective. Front. Public Health 2022; 10: 906788. https://doi.org/10.3389/fpubh.2022.906788
- HOUSE-Colégio F3, ULisboa. Saúde e estilos de vida dos estudantes universitários à entrada da universidade: Relatório do Estudo HOUSE-Colégio F3, ULisboa. Universidade de Lisboa; 2022.
- Teixeira CBC, Moreira DNB. Aplicação de um inventário de saúde mental à população universitária em Portugal: Relatório eesumo do estudo colaborativo entre a RYSE e a ANEP; 2023.
- Gago JS, Andrade MG, Martins MJ, et al. Programa para a promoção da saúde mental no Ensino Superior – Acessibilidade, cooperação e conexões para a promoção da saúde mental no Ensino Superior. República Portuguesa; 2023.
- Alunos matriculados no ensino superior: total e por sexo; 2023. Available online: https://www.pordata.pt/Portugal/Alunos+matriculados+no+ensino+superior+total+e+por+sexo-1048
- Garrido MV, Prada M. Manual de competências académicas. Edições Sílabo; 2016.
- Gaspar T, Correia M, Machado MC, et al. Healthy Workplace Ecosystems (EATS): An assessment tool for healthy workplaces. Revista Psicologia, Saúde & Doenças 2022; 23(1): 252-268. https://doi.org/10.15309/22psd230124
- Burton WHO healthy Workplaces Framework and Model: Background and Supporting Literature and Practice. World Health Organization; 2010.
- Lovibond SH, Lovibond PF. Manual for the Depression, Anxiety, Stress Scales Australia. Psychology Foundation of Australia; 1995.
- Pais-Ribeiro JL, Honrado A, Leal I. Contribuição para o estudo da adaptação portuguesa das escalas de Ansiedade, Depressão e Stress (EADS) de 21 itens de Lovibond e Lovibond. Psicol Saúde Doenças 2004; 5(1): 229-239.
- Cohen J. The Effect Size. In: Statistical Power Analysis for the Behavioral Sciences, 2nd ed. Lawrence Erlbaum Associates; 1988. pp. 77–83.
- Pais-Ribeiro J, Marques T. A avaliação do stresse: A propósito de um estudo de adaptação da escala de percepção de stresse. Psicologia, Saúde e Doenças 2009; 10: 237-248.
- Gaspar T, Tomé G, Cerqueira A, et al. Mental mealth and interpersonal relationships impact in psychological and physical symptoms during adolescence. Revista de Humanidades y Ciencias Sociales 2020; 10: 147-164. https://doi.org/10.33776/erebea.v10i0.495
- Gaspar T, Gaspar S, Guedes F, et al. Study of social and personal factors related to depressive symptoms in adolescence in the COVID-19 Pandemic. Análisis y Modificación de Conducta 2022; 48(177): 3-17 https://doi.org/10.33776/amc.v48i177.7115
- Gaspar T, Paiva T, Matos MG. Ecological Model Explaining the Psychosocial Adaptation to COVID-19. International Journal of Environmental Research and Public Health 2022; 19(9): 5159. https://doi.org/10.3390/ijerph19095159
- Goldberg JM, Sklad M, Elfrink TR, et al. Effectiveness of interventions adopting a whole school approach to enhancing social and emotional development: a meta-analysis. European Journal of psychology of Education 2019; 34: 755-782. https://doi.org/10.1007/s10212-018-0406-9
- Gaspar T, Rebelo A, Mendonça I, et al. Subjective wellbeing and school failure in children and adolescents: Influence of psychosocial factors. International Journal of Development Research 2014; 4(11): 2194-2199.
- Gaspar T, Bilimória H, Albergaria F, et al. Children with special education needs and subjective well-being: Social and personal influence. International Journal of Disability, Development and Education 2016; 63(5): 500-513.
- Barry MM, Clarke AM, Dowling K. Promoting social and emotional wellbeing in schools. Health Education 2017; 117(5): 434–451.
- Tomé G, Almeida A, Ramiro L, et al. Intervention in schools promoting mental health and well-being: a systematic review. Global Journal of Community Psychology Practice 2021; 12(1).