
Healthy Aging: Nutrition and Fitness Tips for Menopausal Women in Asia
- M Fidel Ganis Siregar
- Immanuel Dio L Tobing
- Selly Azmeila
- Corry Carolina Sihombing
- Nabila
- 451-460
- Jun 6, 2024
- Health
Healthy Aging: Nutrition and Fitness Tips for Menopausal Women in Asia
M Fidel Ganis Siregar1,2, Immanuel Dio L Tobing1, Selly Azmeila3, Corry Carolina Sihombing3, Nabila1
1Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Sumatera, Medan, Indonesia
2Fertility and Endocrinology Reproduction Division, Department of Obstetrics and Gynecology, Faculty of Medicine,
Universitas Sumatera, Medan, Indonesia
3Department of Physiology, Faculty of Medicine, Universitas Sumatera, Medan, Indonesia
DOI: https://doi.org/10.51244/IJRSI.2024.1105030
Received: 14 April 2024; Accepted: 09 May 2024; Published: 06 June 2024
ABSTRACT
Menopause represents a significant physiological transition in women, marked by the cessation of menstrual cycles due to declining ovarian function. This narrative review delves into the multifaceted aspects of menopause, focusing on its impact on health, particularly in terms of nutrition, body composition, bone health, cardiovascular risks, and the role of exercise. Four databases were used using MeSH Words “Nutrition” AND “Exercise” AND “Menopause”. A total of 28 studies were included. The transition to menopause involves hormonal changes, notably decreased estrogen levels, leading to various health challenges such as metabolic syndrome, cardiovascular diseases, and osteoporosis. Nutritional strategies play a crucial role during this phase, emphasizing balanced nutrition, adequate protein intake, glycemic index considerations, calcium and vitamin D supplementation, and adherence to dietary patterns like the Mediterranean diet and soybean consumption. Additionally, exercise interventions, including programs like Senam Lansia, offer significant benefits in maintaining cardiovascular fitness, muscle strength, and overall well-being in postmenopausal women. Comprehensive healthcare for menopausal women necessitates a tailored approach encompassing dietary modifications, physical activity, and lifestyle adjustments to optimize health outcomes and mitigate associated risks.
Keywords: Nutrition, Exercise, Menopause, Hormonal changes, Postmenopausal health
INTRODUCTION
Menopause refers to the cessation of menstruation and encompasses the permanent stoppage of menstrual cycles following the decline in ovarian follicular activity[1]. The transition towards menopause, known as the climacteric phase, initiates from the onset of ovarian aging until its completion[2].Throughout this progression, a series of endocrine alterations characterize the gradual loss of ovarian function, primarily marked by reduced levels of ovarian steroids. Declining progesterone levels due to missed ovulation may lead to irregular menstruation and heavy bleeding in the late premenopausal stage. Subsequently, diminishing estradiol levels owing to follicular depletion correlate with vasomotor symptoms, urogenital atrophy, bone density loss, and heightened cardiovascular and metabolic risks. Although menopause represents a noticeable event, its transition might extend over several years, and the health implications of estrogen deficiency can persist for decades, even beyond the absence of apparent symptoms[3].
Menopause associates with an increased likelihood of obesity, metabolic syndrome, cardiovascular ailments, and osteoporosis[3].Weight gain during midlife among women is attributed to both chronological aging and the menopausal shift. Studies reveal that sedentary behavior, rather than menopause itself, significantly increases the risk of overweight or obesity[4,5].Hence, recommending exercise combined with calorie restriction becomes crucial for postmenopausal women dealing with excess weight, aiming to reduce metabolic and cardiovascular risks. Metabolic flexibility, defined as the ability to switch between fat and carbohydrate utilization, may be regulated by gonadal hormones at the mitochondrial level [6]. Postmenopausal women experience reduced metabolic flexibility due to estrogen decline, leading to increased fat accumulation in central regions. Comprehensive healthcare for menopausal women emphasizes lifestyle evaluation and guidance to counteract estrogen deficiency’s adverse effects on general well-being and minimize risks like metabolic syndrome, osteoporosis, fractures, and vascular issues. Nutritional habits hold essential significance during this period, as they impact all women, are modifiable, and influence both longevity and quality of life. This narrative review aims to explore current evidence on the association of dietary patterns with clinical outcomes in postmenopausal women and provide insights into the formulation of optimal dietary guidelines for healthy postmenopausal women. The search strategy was conducted through four databases (Cochrane, PubMed, ScienceDirect, and Google Scholar) using Medical Subject Headings for “Nutrition” AND “Exercise” AND “Menopause”. This narrative review was restricted tofull accessed, quantitative or qualitative studies that were published between 2014 and 2024, which described the correlation between dietary intervention and clinical outcomes in postmenopausal women. 28 studies were included in total. This narrative review will provide informations related to the factors associated with nutritional intake in menopausal women, basic principle of nutrition in menopausal women, dieatary protein, dietary intake and fat mass, vitamin D and calcium, cardioprotective diet, mediterranean dieatary pattern, and exercise in menopausal women.
A. Factors Associated with Nutritional Intake in Menopausal Women
There are several factors that influence nutritional status in menopausal women, including [7]:
- Decreased hormones
Decreased estrogen levels can cause changes in the intestines to slow down, resulting in bowel problems such as constipation. Low estrogen and parathyroid hormones cause calcification of the bones (decalcification), meaning the bones lack potassium so they become porous and break easily. Decreased production of the hormones insulin and thyroxine causes changes in the body’s metabolism. Changes in metabolism, a decrease in estrogen, and a decrease in the release of parathyroid hormone cause changes in the heart and blood vessel system.
- Nutrition
Balanced nutrition is very necessary to meet the body’s needs for energy, focusing on protein, additional calcium, vitamin, and phytoestrogen.
B. Basic Principles of Nutrition in Menopausal Women
Menopause is categorized within the nutritionally vulnerable group, although it is not related to body growth; instead, it ideally involves involution and degeneration of tissues and cells. The vulnerability to nutritional conditions arises from physical conditions, both anatomical and functional. The function and glands of the digestive system have decreased, making foods that are easily digestible and non-burdensome beneficial for the digestive glands. Foods with lower fat content are generally easier to digest but should contain sufficient protein and carbohydrates. Balanced nutrition entails meeting daily nutritional needs with food substances containing carbohydrates, protein, fats, vitamins, minerals, and water. The nutritional requirements for adults with normal weight are around 2000-2200 kcal per day. With this balanced nutrition, it is hoped that individuals will not experience excessive or insufficient body weight and will also avoid conditions such as diabetes mellitus or anemia [7].
If balanced nutrition is adequately consumed, specific nutritional intake to prevent disturbances is not necessary. However, it is not harmful to anticipate the necessary food requirements during menopause or the cessation of estrogen hormones in the body. Especially if there is a risk of certain bodily disturbances that may occur in the future. These types of foods include phytoestrogen-containing foods, such as soybeans or papayas. Additionally, it’s important to consume foods rich in vitamin D, such as tuna, salmon, fish oil, eggs, and milk, although vitamin D can be easily obtained from sunlight [7,8].
Basically, nutritional sufficiency during menopause is similar to nutritional adequacy in younger age groups. The only exception is the decrease in energy requirements that accompany aging. The required foods during menopause are not actually too many. The dietary pattern should also not be the same as in the 30-40 age range because the nutritional needs are clearly different. Eating healthy foods according to individual needs supports a quality life for women in menopause. Caloric and nutritional needs for menopausal women should be tailored according to factors such as weight, height, age, and activity level, which generally are lower compared to adult requirements. The basic principles to fulfill nutrition in menopausal women include [7,8]:
- Providing a diet appropriate to the disease alongside treatment
- Consuming blood supplements to address anemia
- Consuming non-fat milk/foods high in calcium to counteract osteoporosis
- Consuming sufficient fiber (vegetables and fruits) to address constipation
- Regular exercise
- Limiting sodium intake found in packaged foods, usually in snacks often consumed.
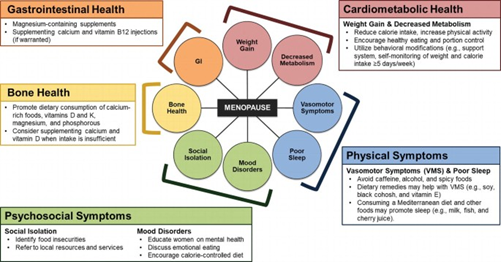
Fig 1. Dietary consideration for menopausal women [7,8]
TABLE I A sample menu dedicated to a menopausal woman [9]
| Patient’s details | |
| Patient’s body weight: 93 kg Height: 165 cm Age: 54 Low physical activity (daily activities): PAL = 1.4 BMI = 34.19 kg/m2 (grade 1 obesity) |
|
| Step 1. Estimating energy requirement (Harris-Benedict equation) | |
| BMR (kcal) = 655.1 + (9.563 x weight [kg]) + (1.85 x height [cm]) – (4.676 x age [years]) BMR (kcal) = 655.1 + 9.563 x 93 + 1.85 x 165 – 4.676 x 54 BMR (kcal) = 655.1 + 889.3 x 305.25 – 252.5 BMR (kcal) = 1597.15 |
|
| TMR (kcal) = BMR x physical activity level TMR (kcal) = 1597.15 x 1.4 TMR (kcal) = 2236 kcal |
|
| Assumed calorie reduction of a daily menu – 636 kcal | |
| Diet energy value after reducing an estimated calorie level amounts to: Energy = 1600 kcal |
|
| Step 2. Estimating protein (P) requirement | |
| Protein should constitute 20-25% of a diet energy value. P = 20% x 1600 kcal = 320 kcal 1 g protein = 4 kcal P = 320 kcal/4 kcal = 80 g |
|
| Step 3. Estimating fat (F) requirement | |
| Fat should constitute 20-25% of a diet energy value. F = 25% x 1600 kcal = 400 kcal 1 g fat = 9 kcal F = 400 kcal/9 kcal = 44.5 g |
|
| Step 4. Estimating carbohydrates (C) requirement | |
| Carbohydrates supplement a diet energy value. C (percentage) = 100% – (20% + 25%) = 100% – 45% = 55% C = 55% x 1600 kcal = 880 kcal 1 g carbohydrates = 4 kcal C = 880 kcal/4 kcal = 220 g |
|
| Dietary fiber: 30 g | |
| Diet plan nutritional information | |
| Energy = 1600 kcal Protein = 80 g Fat = 44.5 g Carbohydrates = 220 g |
1st breakfast 25% kcal = 400 kcal 2nd breakfast 10% kcal = 160 kcal Dinner 35% kcal = 560 kcal Afternoon snack 10% kcal = 160 kcal Supper 20% kcal = 320 kcal |
C. Dietary Protein
Aging induces an elevation in the body’s requirement for dietary protein due to a decline in the ability of skeletal muscles to activate protein synthesis in response to stimuli that promote growth, potentially influenced by insulin resistance. A study conducted by Gregorio et al. showed that the older postmenopausal women who consumes 25% protein less than the recommended daily allowance (RDA) had higher body fat and fat-to-lean ratio than those who consumed the higher protein diet [10].Observational investigations have suggested a link between higher protein consumption and increased lean body mass (LBM) among postmenopausal women. For instance, in the Women’s Health Initiative study, a higher protein intake of 1.2 grams per kilogram of body weight was associated with a 32% decreased risk of frailty and improved physical function [11]. Postmenopausal women exhibited elevated skeletal muscle mass index with a mean protein intake of 1.6 grams per kilogram of body weight, while the Institute of Medicine recommends a protein allowance of 0.8 grams per kilogram of body weight for all age groups. However, observational findings cannot establish causation, prompting the development of randomized controlled trials (RCTs) to substantiate this notion [7].
A meta-analysis encompassing 36 RCTs involving 1682 participants found that protein supplementation over periods ranging from 6 to 78 weeks did not result in increased LBM among non-frail older adults living in the community. Limited interventional studies focusing on Section Headings postmenopausal women have indicated that a higher intake of protein did not facilitate gains in LBM when compared to the recommended dietary allowance (RDA) [12].
D. Dietary Intake and Fat Mass
Based on a recent RCT of 57 overweight and obese women, low-carbohydrate-high-fat diet had no superior effect on fat mass in comparison to a normal diet [13]. It is necessary to consider other ways to characterize carbohydrate foods, such as fiber, whole grain content, glycemic index (GI) should also be considered particularly important in reducing total body fat mass and managing weight. Eating a meal with high GI elicits a quick pancreatic response to the rising blood glucose levels, with intense insulin secretion that rapidly lowers blood glucose and causes hunger and overeating. In fact, a Cochrane systematic review including data from 202 overweight or obese men and women in six RCTs reported a significantly greater decrease in total fat mass in the low GI diet than in control diet group. Specifically in postmenopausal women, a clinical trial with low GI (<55) dietary intervention, aimed to balance energy needs, has shown that, despite similar energy intake and resting metabolic rates during the six months of follow-up, all participants lost total body and regional fat mass [14, 15].
E. Vitamin D and Calcium
The decline in bone mineral density (BMD) observed during aging is closely associated with decreasing concentrations of reproductive hormones. The reduction in BMD accelerates notably during the late perimenopausal period, characterized by increasingly irregular menstrual cycles. Various studies have underscored the significance of adequate intake of calcium and vitamin D in promoting better BMD and preventing osteoporosis and fractures in older individual. However, recommended daily calcium intake for older adults varies from 700 mg in the UK to 1200 mg in the US, with the North American Menopause Society recommending a dietary calcium intake of 1000 to 1500 mg per day specifically for postmenopausal women. Daily supplementation with both vitamin D (400–800 IU/day) and calcium (1000–1200 mg/day) has shown more promise as a strategy [16, 17].A recent meta-analysis demonstrated that combined calcium and vitamin D significantly increased total bone mineral density and prevent the incidence of osteoporosis hip fracture in postmenopausal women [18].
F. Cardioprotective Diet
Diet represents a significant controllable factor influencing cardiovascular disease (CVD) risk. In conventional nutritional epidemiology, the focus lies on assessing the potential effects of specific foods or nutrients [19, 20]. Leading scientific organizations propose a healthy dietary regimen aiming to reduce the risk of major chronic ailments and enhance overall health. This regimen advocates for obtaining protein mainly from plant-based sources, nuts, fish, or alternative omega-3 fatty acid sources; acquiring fats primarily from unsaturated plant origins; obtaining carbohydrates mainly from whole grains; consuming a minimum of five servings of fruits and vegetables daily; and considering moderate dairy intake as an option [21]. The American Heart Association (AHA) outlines specific dietary objectives to enhance cardiovascular health, including daily intake goals such as≥ 4.5 cups of fruits, ≥ 200 grams of fish and shellfish per week, limiting sodium to ≤ 1500 milligrams per day, restricting sugar-sweetened beverages to ≤ 36 fluid ounces per week, consuming three or more 1-ounce-equivalent servings of whole grains per day, and consuming at least four servings of nuts, seeds, and legumes weekly [22].
G. Mediterranean Dietary Pattern
Mediterranean diet is a nutritious eating plan characterized by sufficient intake of vegetables, fruits, whole grains, and legumes with a replacement of saturated animal fats in favor of unsaturated vegetable fat[23]. It has been associated with improved muscle measurements in postmenopausal women by directly influencing oxidative stress, inflammation, and insulin resistance—factors known to contribute to muscle breakdown. Granic et al., in a recent review, put forth the hypothesis that the mediterranean diet’s ‘myoprotective’ effect may be attributed to a higher intake of plant-based foods, as these contain a combination of nutrients that collectively aid in preserving muscles. In a prior study, we also proposed a model outlining the potential advantages of the mediterranean diet concerning body composition in postmenopausal women. This diet’s components, such as antioxidants like beta-carotene, along with vitamins C and E, serve to shield against the harmful effects of oxidative stress, while the presence of magnesium enhances energy metabolism, transmembrane transport, and skeletal muscle functionality [24, 25].
A prospective cohort study which investigated six different dietary patterns stated that Mediterranean style diet inversely associated with vasomotor menopausal symptoms such as hot flushes and night sweats [26]. A randomized controlled trial was conducted in Spain to determine whether the Mediterranean diet (MedD) was superior to a low-fat diet. The study included 7447 participants, consisting of older men and postmenopausal women with CVD risk factors. The MedD group was supplemented with virgin oil or mixed nuts and compared it to the low-fat diet. The incidence of major cardiovascular events was lower among those assigned to a Mediterranean diet[27]. The similar study also observed the adjusted difference in 5-year changes in waist circumference was -0·466 cm (-1·109 to 0·176; p = 0·154) in the MedDiet with olive oil group and -0·923 cm (-1·604 to -0·241; p = 0·008) in the MedD with nut group, compared with the control group [27]. In terms of decreasing obesity and cardiovascular and metabolic events, the Mediterranean diet and pharmacological interventions are comparable [28].
Utilization of Soybeans in Asian Diets
Soybeans possess an exceptional nutritional and functional food profile owing to their composition. Largely devoid of starch, soybeans hold significance within diabetic diets. They boast high levels of protein, carbohydrate conjugates, fatty acids, soybean oil, and amino acids, contributing to their nutritional richness. Furthermore, soybeans contain a spectrum of biologically relevant phytochemicals as minor components, encompassing both organic and inorganic constituents such as minerals. Each component within soybeans exerts discernible impacts on human health and can be extracted utilizing various techniques. Considering their nutrient composition, soybeans and related foods have been acknowledged for their nutritional value and potential health benefits in humans [29].
Emerging evidence underscores the significant health implications associated with the consumption of soy foods. Isoflavone-rich soybeans, frequently included in Asian diets, correlate with a reduced incidence of menopausalsymptoms, osteoporosis, cardiovascular diseases, and hormone-dependent cancers. Recent cohort study with multivariable-adjusted analysis discovered that isoflavone intake was inversely associated with coronary heart disease in young women or postmenopausal women without hormone use [30].Moreover, an evident association exists between increased consumption of soybeans and a lowered risk of cancer development. Epidemiological investigations have delved into the association between soybean consumption and diminished vasomotor symptoms. However, a systematic review by Thomas et al. concluded that synthetic isoflavone may have been more effective in reducing the symptom of hot flush compared to soy isoflavone [31].Consumption of soybeans is notably higher in Asian nations like China, Japan, Taiwan, and Korea compared to Western countries. Notably, postmenopausal Asian women exhibit significantly lower occurrences (10–25%) of hot flashes in contrast to their counterparts in Western countries, where rates range between 60–90% [29]. Furthermore, additional research is needed to examine the isoflavones found in soybeans and their impact on health in postmenopausal women.
H. Exercise
During the transition to menopause, women undergo simultaneous decreases in their basal metabolic rate and lean muscle mass. While weight gain during midlife is commonly linked to menopause, it is primarily influenced by age rather than menopause itself. On average, midlife women tend to gain approximately 4.5 to 4.9 pounds over a span of three years. Reduced estrogen levels during menopause are linked to an increase in abdominal and visceral fat if there is no simultaneous change in physical activity or overall body weight, leading to a shift toward an android pattern of fat distribution and a rise in total body fat among women. The accumulation of abdominal fat in postmenopausal women is a critical factor in the development of insulin resistance, a key risk factor associated with the onset of type 2 diabetes. Additionally, postmenopausal abdominal weight gain is associated with an unfavorable lipid profile, marked by an increase in low-density lipoprotein cholesterol and a decrease in the ratio of total cholesterol to high-density lipoprotein cholesterol. Exercise has the potential to reverse or mitigate the aforementioned effects of aging and menopause [31].
The American Heart Association (AHA) and the American College of Sports Medicine offer exercise recommendations for individuals aged 65 and above. Notably, these guidelines are derived from laboratory training data and lack direct observations in real-life conditions. The exercise recommendations encompass four primary categories of physical fitness: aerobic exercise, muscle strengthening, flexibility, and balance. Aerobic exercise involves engaging large muscle groups and should be sustained for at least 10 minutes. Examples include brisk walking, swimming, tennis, water aerobics, dancing, and cycling [31].A systematic review by Loaiza-Betancur et al., stated that exercise training resulted in clinically significant reductions on systolic and diastolic blood pressure, and combining exercise training with aerobic training generated larger reductions in menopausal and postmenopausal women, with prehypertension or hypertension[32].
Muscle strength is developed through weight training, resistance exercises, or weight-bearing calisthenics. Muscle-strengthening activities should be performed at least twice a week on non-consecutive days, targeting 8 to 10 major muscle groups (such as abdomen, bilateral arms, legs, shoulders, and hips). Aim to complete 10 to 15 repetitions of each exercise at an intensity between 60% to 75% of the maximum one-repetition effort, gradually increasing resistance over time. Flexibility exercises, including stretching and yoga, are essential for everyday tasks such as reaching overhead or tying shoelaces. Balance exercises improve stability and may help prevent falls or reduce fall-related injuries. The advantages of regular physical activity include reduction in risk of cardiovascular events, reduction in obesity, diminished risk of hypertension and diabetes mellitus, improvement in blood lipid profile, reduction in risk of cancer, and many others [31, 33]. A meta-analysis encompassing 21 RCTs involving 2884 participants found that exercise is also significantly improved severity of vasomotor symptoms[34].
Senam Lansia, an Indonesian exercise for elderly people, is a light and easy exercise that is not a burdensome activity designed specifically for elderly individuals. The movements are suitable for elderly people, such as avoiding jump, jumping, crossing legs, walking back and forth, and jerking, but they still have the potential to stimulate the heart and lungs at a light to medium intensity. The majority of the body’s muscles are involved in the movements, which are harmonious based on daily movements and provide balance between the right and left part of the body. This sporting activity will help the body stay fit and fresh because it trains the bones to stay strong. This sporting activity will help the body stay fit and fresh because it trains the bones to stay strong. It also encourages the heart to work optimally and assists in eliminating free radicals that are present in the body thereby increasing the immune system. The assessment of fitness level involves the heart rate, also known as the pulse rate at rest. In order to be healthier, it’s necessary to decrease the resting heart rate. The principles of elderly exercise are [35]:
- The movement is dynamic (changing)
- Progressive (gradually increasing)
- There is a warm-up and cool-down for each exercise
- The duration of exercise lasting 15-30 minutes is the time or duration required each time you practice, to improve lung-heart fitness and reduce weight. The duration of sports training to get good results for cardiovascular function is to reach the training zone area and last up to 15 – 45 minutes.
- The minimum frequency of training per week is 3 times and optimally 5 times. The number of training units per week, to improve fitness you need to train 3 – 5 times per week. Training 6 – 7 times per week is not recommended because the body needs sufficient recovery to maintain physical fitness
CONCLUSION
In conclusion, navigating the complexities of menopause requires a comprehensive approach that encompasses nutrition, exercise, and awareness of hormonal changes. The transition to menopause brings about significant physiological alterations, including hormonal shifts that can impact various aspects of health. Adequate nutrition, with a focus on balanced meals rich in essential nutrients like calcium and vitamin D, plays a crucial role in supporting bone health and managing metabolic changes. Incorporating regular exercise, tailored to individual needs and abilities, helps mitigate the effects of aging and hormonal fluctuations, promoting overall well-being and cardiovascular health. Understanding these key factors and implementing appropriate lifestyle adjustments can empower women to navigate menopause with resilience and maintain optimal health throughout their postmenopausal years.
REFERENCES
- World Health Organizations. Menopause [Internet]. 2022 [cited 2024 Apr 5]. Available from: https://www.who.int/news-room/fact-sheets/detail/menopause
- Blümel JE, Lavín P, Vallejo MS, Sarrá S. Menopause or climacteric, just a semantic discussion or has it clinical implications? Climacteric. 2014;17(3):235–41.
- El Khoudary SR, Aggarwal B, Beckie TM, Hodis HN, Johnson AE, Langer RD, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. 2020 Dec 22;142(25):e506–32.
- Blümel JE, Fica J, Chedraui P, Mezones-Holgún E, Zuñiga MC, Witis S, et al. Sedentary lifestyle in middle-aged women is associated with severe menopausal symptoms and obesity. Menopause. 2016;23(5):488–93.
- de Araújo, M do ESC, da Conceição Chagas de Almeida M, Matos SMA, de Jesus Mendes da Fonseca M, Pitanga CPS, Pitanga FJG. Combined Effect of Leisure-Time Physical Activity and Sedentary Behavior on Abdominal Obesity in ELSA-Brasil Participants. Int J Environ Res Public Health. 2023;20(15):1–12.
- Eaton SA, Sethi JK. Immunometabolic Links between Estrogen, Adipose Tissue and Female Reproductive Metabolism. Biology (Basel). 2019 Feb 7;8(1):8.
- Ten Haaf DSM, Nuijten MAH, Maessen MFH, Horstman AMH, Eijsvogels TMH, Hopman MTE. Effects of protein supplementation on lean body mass, muscle strength, and physical performance in nonfrail community-dwelling older adults: a systematic review and meta-analysis. Am J Clin Nutr. 2018 Nov 1;108(5):1043–59.
- Marlatt KL, Gilmore LA, Flanagan EW, Redman LM. Dietary Considerations for Postmenopausal Women. In: Wilson T, Temple NJ, Bray GA, editors. Nutrition Guide for Physicians and Related Healthcare Professions [Internet]. Cham: Springer International Publishing; 2022 [cited 2023 Dec 20]. p. 71–82. (Nutrition and Health).
- Brończyk-Puzoń A, Piecha D, Nowak J, Koszowska A, Kulik-Kupka K, Dittfeld A, et al. Guidelines for dietary management of menopausal women with simple obesity. Przegla̜d Menopauzalny = Menopause Review. 2015 Mar;14(1):48.
- Gregorio L, Brindisi J, Kleppinger A, Sullivan R, Mangano KM, Bihuniak JD, et al. Adequate dietary protein is associated with better physical performance among post-menopausal women 60-90 years. J Nutr Heal Aging. 2014;18(2):155–60.
- Silva TR, Spritzer PM. Skeletal muscle mass is associated with higher dietary protein intake and lower body fat in postmenopausal women: a cross-sectional study. Menopause. 2017 May;24(5):502–9.
- Rossato LT, Nahas PC, de Branco FMS, Martins FM, Souza AP, Carneiro MAS, et al. Higher Protein Intake Does Not Improve Lean Mass Gain When Compared with RDA Recommendation in Postmenopausal Women Following Resistance Exercise Protocol: A Randomized Clinical Trial. Nutrients. 2017 Sep 12;9(9):1007.
- Valsdottir TD, Øvrebø B, Falck TM, Litleskare S, Johansen EI, Henriksen C, et al. Low-carbohydrate high-fat diet and exercise: Effect of a 10-week intervention on body composition and cvd risk factors in overweight and obese women—a randomized controlled trial. Nutrients. 2021;13(1):1–25.
- Silva LRD, Vargas RF, Shinzato JY, Derchain SFM, Ramalho S, Zeferino LC. Association of Menopausal Status, Expression of Progesterone Receptor and Ki67 to the Clinical Response to Neoadjuvant Chemotherapy in Luminal Breast Cancer. Rev Bras Ginecol Obstet. 2019 Dec;41(12):710–7.
- Augustin LSA, Kendall CWC, Jenkins DJA, Willett WC, Astrup A, Barclay AW, et al. Glycemic index, glycemic load and glycemic response: An International Scientific Consensus Summit from the International Carbohydrate Quality Consortium (ICQC). NutrMetab Cardiovasc Dis. 2015 Sep;25(9):795–815.
- North American Menopause Society. The role of calcium in peri- and postmenopausal women: 2006 position statement of the North American Menopause Society. Menopause. 2006;13(6):862–77; quiz 878–80.
- Silva TR, Oppermann K, Reis FM, Spritzer PM. Nutrition in Menopausal Women: A Narrative Review. Nutrients. 2021 Jun 23;13(7):2149.
- Liu C, Kuang X, Li K, Guo X, Deng Q, Li D. Effects of combined calcium and vitamin D supplementation on osteoporosis in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Food Funct. 2020;11(12):10817–27.
- Oppermann K, Colpani V, Spritzer PM. Risk factors associated with coronary artery calcification in midlife women: a population-based study. Gynecol Endocrinol. 2019 Oct;35(10):904–8.
- Maas AHEM, Rosano G, Cifkova R, Chieffo A, van Dijken D, Hamoda H, et al. Cardiovascular health after menopause transition, pregnancy disorders, and other gynaecologic conditions: a consensus document from European cardiologists, gynaecologists, and endocrinologists. Eur Heart J. 2021 Jan 25;42(10):967–84.
- Hallajzadeh J, Khoramdad M, Izadi N, Karamzad N, Almasi-Hashiani A, Ayubi E, et al. Metabolic syndrome and its components in premenopausal and postmenopausal women: a comprehensive systematic review and meta-analysis on observational studies. Menopause. 2018 Oct;25(10):1155–64.
- Willett W, Rockström J, Loken B, Springmann M, Lang T, Vermeulen S, et al. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet. 2019 Feb 2;393(10170):447–92.
- Pugliese G, Barrea L, Laudisio D, Aprano S, Castellucci B, Framondi L, et al. Mediterranean diet as tool to manage obesity in menopause: A narrative review. Nutrition [Internet]. 2020;79–80:110991. Available from: https://doi.org/10.1016/j.nut.2020.110991
- Granic A, Sayer AA, Robinson SM. Dietary Patterns, Skeletal Muscle Health, and Sarcopenia in Older Adults. Nutrients. 2019 Mar 30;11(4):745.
- Baumann CW, Kwak D, Liu HM, Thompson LV. Aging and Exercise: Age-induced oxidative stress: how does it influence skeletal muscle quantity and quality? Journal of Applied Physiology. 2016 Nov 11;121(5):1047.
- Herber-Gast GCM, Mishra GD. Fruit, Mediterranean-style, and high-fat and -sugar diets are associated with the risk of night sweats and hot flushes in midlife: Results from a prospective cohort study. Am J Clin Nutr [Internet]. 2013;97(5):1092–9. Available from: https://doi.org/10.3945/ajcn.112.049965
- Estruch R, Ros E, Salas-Salvadó J, Covas M-I, Corella D, Arós F, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med. 2018;378(25):1–14.
- Barrea L, Pugliese G, Laudisio D, Colao A, Savastano S, Muscogiuri G. Mediterranean diet as medical prescription in menopausal women with obesity: a practical guide for nutritionists. Crit Rev Food Sci Nutr [Internet]. 2021;61(7):1201–11. Available from: https://doi.org/10.1080/10408398.2020.1755220
- Chen LR, Chen KH. Utilization of Isoflavones in Soybeans for Women with Menopausal Syndrome: An Overview. Int J Mol Sci. 2021 Mar 22;22(6):3212.
- Ma L, Liu G, Ding M, Zong G, Hu FB, Willett WC, et al. Isoflavone Intake and the Risk of Coronary Heart Disease in US Men and Women: Results from 3 Prospective Cohort Studies. Circulation. 2020;141(14):1127–37.
- Grindler NM, Santoro NF. Menopause and exercise. Menopause. 2015 Dec;22(12):1351.
- Loaiza-Betancur AF, Chulvi-Medrano I, Díaz-López VA, Gómez-Tomás C. The effect of exercise training on blood pressure in menopause and postmenopausal women: A systematic review of randomized controlled trials. Maturitas. 2021;149(May):40–55.
- Sternfeld B, Guthrie KA, Ensrud KE, LaCroix AZ, Larson JC, Dunn AL, et al. Efficacy of exercise for menopausal symptoms: a randomized controlled trial. Menopause. 2014 Apr;21(4):330–8.
- Liu T, Chen S, Mielke GI, McCarthy AL, Bailey TG. Effects of exercise on vasomotor symptoms in menopausal women: a systematic review and meta-analysis. Climacteric. 2022 Dec;25(6):552-561. doi: 10.1080/13697137.2022.2097865. Epub 2022 Jul 29. PMID: 35904028.
- Handayani S, Haris A. Pengaruh Senam Lansia Terhadap Aktivitas Sehari-Hari Lansia Di Desa Puyung Wilayah Kerja Puskesmas Puyung Kecamatan Jonggat Kabupaten Lombok Tengah Tahun 2017