
Determinants of cervical cancer screening among women aged 25 to 65 years in a semi-rural area in Cameroon
- Ngon Emmanuel Wasibang
- Simo Wambo Andre
- Tchounzou Robert
- 542-556
- Apr 18, 2025
- Education
Determinants of Cervical Cancer Screening among Women Aged 25 to 65 Years in a Semi-Rural Area in Cameroon
Ngon Emmanuel Wasibang*, Simo Wambo Andre, and Tchounzou Robert
University of Buea
*Corresponding author
DOI: https://doi.org/10.51244/IJRSI.2025.121500050P
Received: 06 March 2024; Accepted: 11 March 2025; Published: 18 April 2025
ABSTRACT
Background: Cervical cancer is the fourth most common cancer globally and the second leading cause of cancer-related deaths among women in low- and middle-income countries. Screening is a critical prevention and control strategy. This study investigates the factors influencing the uptake of cervical cancer screening services among women aged 25-65 in Kumba, Cameroon.
Methods: A cross-sectional study was conducted in Kumba, involving 400 women aged 25-65 years who provided informed consent. Data were collected using a structured questionnaire, divided into four sections: knowledge of cervical cancer, uptake of cervical cancer screening, and factors facilitating or hindering screening. Data were analyzed using SPSS version 26, and inferential statistical analyses, including logistic regression, were performed to identify determinants of cervical cancer screening uptake. Results were presented in tables and figures.
Results: The mean age of participants was 33.78 years, with the majority (64.3%) between 25-29 years. 64.0% of participants had adequate knowledge of cervical cancer, while 43.0% reported having undergone cervical cancer screening. Women residing in the Kumba Town Health Area were more likely to participate in screening compared to those in the Fiango Health Area (AOR=2.55, CI=1.20-5.44, p value= 0.023). Women aged 35-44 years were more likely to undergo screening than those aged 25-34 years (AOR=1.96, CI=1.03-3.71, p value=0.041). Adequate knowledge of cervical cancer was associated with a higher likelihood of screening uptake (AOR=2.96, CI=1.56-5.59, p value=0.003). Additionally, having a relative who had been screened increased the likelihood of participation in screening by 3.8 times (AOR=3.82, CI=2.08-7.00, p value=<0.000).
Conclusions: This study identified key determinants of cervical cancer screening uptake, including age (35-44 years), adequate knowledge of cervical cancer, and having a screened relative. The results highlight the need for targeted interventions to improve awareness and accessibility of screening services, particularly in under-screened areas like Fiango Health Area. Public health strategies should focus on increasing educational campaigns and encouraging family involvement in screening programs to enhance uptake in similar settings.
Keywords: Kumba, Uptake, Cervical Cancer, Screening, Determinants.
INTRODUCTION
Cervical cancer is a leading cause of cancer-related deaths among women globally, particularly in low- and middle-income countries (LMICs). It is primarily caused by persistent infection with high-risk types of the human papillomavirus (HPV), with types 16 and 18 being the most oncogenic (Okyere et al., 2021; Simo et al., 2021). HPV, a family of double-stranded DNA viruses, is classified into two groups: non-oncogenic (low-risk) and oncogenic (high-risk) types. While low-risk HPV strains can lead to anogenital warts and respiratory infections, high-risk strains are associated with an increased risk of cancers, including cervical, anal, and oropharyngeal cancers (Bencherit et al., 2022; Bedell et al., 2020).
Cervical cancer is unique in that it has a long pre-invasive phase during which precancerous lesions can be detected and treated through screening, preventing progression to invasive disease (Ahmed et al., 2013; Ayenew et al., 2020). Despite being a preventable disease with early detection, cervical cancer remains the fourth most common cancer among women worldwide, with nearly 90% of related deaths occurring in LMICs (Donatus et al., 2019). In Sub-Saharan Africa, where access to screening and treatment remains limited, cervical cancer is a major public health challenge (Balogun et al., 2012; Tadzong-Awasum & Morgan, 2021).
In Cameroon, cervical cancer accounts for approximately 24% of cancer cases among women of reproductive age, yet the uptake of cervical cancer screening remains alarmingly low at only 19.6% (Donatus et al., 2019). The low utilization of screening services is a critical concern, as early diagnosis and treatment are essential for improving survival rates. Factors contributing to the low uptake include limited awareness, cultural barriers, and poor access to healthcare services.
This study aimed to identify the determinants of cervical cancer screening uptake among women aged 25-65 in Kumba, a semi-rural area in Cameroon. Specifically, it assessed women’s knowledge of cervical cancer, determined the level of screening uptake, and identified key factors influencing this uptake. Understanding these determinants is crucial for designing effective public health interventions tailored to local needs. The findings from this study will inform the development of policies and programs to improve the uptake of cervical cancer screening services in Kumba and other areas with similar socio-cultural and healthcare characteristics.
MATERIALS AND METHODS
Study Design
This was a community-based, cross-sectional, analytical study.
Study Duration and Period
The study spanned from October 2023 to June 2024, with data collection occurring between January and April 2024.
Study Area
The study was conducted in Kumba, a major town in the South West Region of Cameroon, divided into Kumba North District (KND) and Kumba South District (KSD). According to epidemiological reports from January to June 2023, KND and KSD had a combined population of 401,239, with KSD’s population roughly double that of KND. KSD comprises seven health areas, while KND has six. Kumba is predominantly inhabited by the Bakossi and Bafaw ethnic groups, among others. Three major facilities in Kumba offer cervical cancer screening services: Kumba Baptist Hospital (Pulletin Health Area, KND), Regional Hospital Annex Kumba (KSD), and Presbyterian Hospital Mayemeng (Kossala, Fiango Health Area, KSD). These facilities offer cervical cancer screening using HPV DNA testing, Pap smears, and visual inspection with acetic acid (VIA) and visual inspection with Lugol’s iodine (VILI), following WHO recommendations. While WHO guidelines recommend screening beginning at age 21, this study adopted the more recent American Cancer Society recommendations, focusing on women aged 25-65.
Target Population
The study included all women aged 25-65 residing in Kumba.
Inclusion and Exclusion Criteria
Women aged 25-65 residing in Kumba who were able to provide informed consent were included. Women unable to answer questions due to serious physical or mental illness were excluded. “Medically fit” in this context refers to the ability to participate in the interview process and provide informed consent, not a clinical assessment of suitability for screening.
Sample Size and Sampling Technique
- Sample Size Determination: The sample size was calculated using Cochran’s formula Where no= minimum sample size required for infinite population z=standard normal deviation 1.96, e2= degree of precision or accuracy (0.05) P= 0.438 level of uptake of cervical cancer screening in Kumbo west district Cameroon is 43.48% (Donatus et al., 2019), q=1-P= 0.565. Hence Sample size (no) = (1.96)2*(0.435)*(0.565)/(0.05) = 378 participants. After 5% correction a mininmum sample size of 400 participants
- Sampling Technique: A multi-stage sampling technique proportionate to size was employed. First, Kumba was divided into KND and KSD. Then, two health areas were randomly selected from KND and three from KSD using balloting. Next, three communities within each selected health area were randomly selected using balloting. Finally, systematic sampling was used to select households, interviewing every third household. In households with multiple eligible women, the eldest was prioritized. This process was repeated across all five health areas to reach the target sample size of 400 (Table 1).
Table 1 Population Distribution Of The Sample Population With Respect To Each Health Area
| DITRICT | HEALTH AREA | POPULATION | PROPORTION | SAMPLE POPULATION |
| KUMBA NORTH | Kumba Pulletine | 3539 | 0.067 | 25 |
| Kumba town. | 15704 | 0.3 | 120 | |
| KUMBA SOUTH | Kumba Station | 2792 | 0.052 | 20 |
| Fiango | 13924 | 0.262 | 105 | |
| Kumba mbeng | 17251 | 0.324 | 130 | |
| Total | Total | 53210 | 100 | 400 |
Data Collection Tool and Procedure
- Data Collection Tool: A structured, self-administered questionnaire with closed-ended questions was used. The questionnaire was divided into four sections: sociodemographic characteristics, knowledge of cervical cancer (which involved 11 questions, with each correctly answered question earning a point, sum of points or scores above 7 indicating adequate knowledge), self-reported cervical cancer screening uptake, and factors influencing uptake. Knowledge questions were adapted from previous studies (Donatus et al., 2019; Moshi et al., 2019; Wakwoya et al., 2020). Knowledge was assessed on cervical cancer awareness, it’s causes, risk factors, symptoms, transmission, information sources, recommended screening age, and prevention methods.
- Data Collection Procedure: Permission was obtained from the District Medical Officer. Community health workers accompanied data collectors (nurses with diplomas or BSc degrees). Participants were informed about the study, questions were clarified, and written informed consent was obtained before administering the questionnaire. Data collectors were present during completion to ensure completeness and accuracy.
Validity and Reliability
- Validity: The questionnaire was reviewed by a gynecologist and an epidemiologist. A pre-test was conducted with 30 women in Konye, and the questionnaire was revised based on the feedback.
- Reliability: Data collectors received three days of training on the study objectives and ethical principles. Training effectiveness was assessed through Q&A sessions. Daily data was checked for accuracy and completeness.
Data Management
Data was entered into Epi Info version 7.2.5, exported to Microsoft Excel for cleaning, and analyzed using SPSS version 26. Univariate, bivariate, and multivariate analyses were performed. Variables with p value < 0.2 in bivariate analysis were included in the multivariate analysis. A p-value ≤ 0.05 in the multivariate analysis indicated a strong statistical association with the dependable variable
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of the Faculty of Health Sciences, University of Buea. Authorization was obtained from the Regional Delegation of Public Health, South West Region, and the District Medical Officers of Kumba North and South. Written informed consent was obtained from all participants.
RESULTS
Socio-Demographic Characteristics
From table 2a: A total of 400 women consented for this study, the mean age and standard deviation of the respondents was 33.78±7.803. The majority of the participants (64.3%) were in the 25-34 years age group with 32.5% living in Kumba Mbeng Health Area. More than one quarter of the participants were private employees (26.5%), with 23.0% of the participants doing business. More than half (53.0%) of the participants had secondary level education.
Table 2a: Distribution of participants based on socio-demographic characteristics
| Variable | Category | Frequency | Percentage (%) |
| Age (years) | 25-34 | 257 | 64.3 |
| 35-44 | 103 | 25.7 | |
| 45-55 | 25 | 6.3 | |
| 55-65 | 15 | 3.7 | |
| Total | 400 | 100.0 | |
| Health Area | Fiango | 105 | 26.3 |
| Kumba mbeng | 130 | 32.5 | |
| Kumba station | 21 | 5.2 | |
| Kumba town | 107 | 26.7 | |
| Pulletine | 37 | 9.3 | |
| Total | 400 | 100 | |
| Occupation | Housewife | 73 | 18.3 |
| Farming | 45 | 11.3 | |
| Business | 92 | 23.0 | |
| Government Employee | 26 | 6.4 | |
| Private Employee | 106 | 26.5 | |
| Student | 56 | 14.0 | |
| Retired | 2 | 0.5 | |
| Total | 400 | 100 | |
| Educational level | Primary | 77 | 19.3 |
| Secondary | 212 | 53.0 | |
| University | 111 | 27.7 | |
| Total | 400 | 100 |
From table 2b; Majority (61.5%) of the participants were married with more than three quarter (87.5%) being Christians. More than one third (35.7%) of the participants had 2-3 children, with more than two third (66.5%) of the participants visiting the health facility more than once a year. About half of the participants (49.5%) had less than 50.000FRS as average monthly incom
Table 2b: Distribution of participants based on socio-demographic characteristics
| Variable | Category | Frequency | Percentage % |
| Marital Status | Married | 246 | 61.5 |
| Single | 136 | 34 | |
| Divorce | 10 | 2.5 | |
| Widow | 8 | 2 | |
| Total | 400 | 100 | |
| Religion | Christianity | 350 | 87.5 |
| Muslim | 22 | 5.5 | |
| African tradition religion | 25 | 6.2 | |
| None | 3 | 0.8 | |
| Total | 400 | 100 | |
| Number of children | No child | 97 | 24.2 |
| One child | 92 | 23 | |
| 2-3 children | 143 | 35.7 | |
| Greater than 3 children | 68 | 17 | |
| Total | 400 | 100 | |
| Average number of time visited hospital | Once a year | 113 | 28.2 |
| More than once a year | 266 | 66.5 | |
| Never visited a health facility | 21 | 5.3 | |
| Total | 400 | 100 | |
| Average monthly income | Less than 50.000 | 198 | 49.5 |
| 50.000-100.000 | 110 | 27.5 | |
| 101.000-150.000 | 48 | 12 | |
| Greater than 150.000 | 44 | 11 | |
| Total | 400 | 100 |
Knowledge Of Participants On Cervical Cancer
Table 3 shows that two-thirds (66.5%) of the participants had heard of cervical cancer, with a similar proportion (66.3%) knowing it is a fatal disease. Less than one-third were unaware that cervical cancer can be fatal. Approximately 43% of participants knew that the human papillomavirus (HPV) causes cervical cancer. A large majority (76%) were aware of cervical cancer screening services.
The most common source of information about cervical cancer was healthcare workers (63.8%), followed by the media (15.7%), community workers (9%), friends/relatives (6.6%), and printed materials (4.8%).
A vast majority (85%) of participants knew that screening can detect cervical cancer early. However, only about 43.8% were aware that screening can begin before the age of 20. While 85% knew that cervical cancer screening is available in hospitals, just over two-thirds (68%) understood that cervical cancer is treatable if detected early.
Table 3: Distribution of participants based on knowledge of cervical cancer
| Variable | Category | Frequency | Percentage % |
| Heard of cervical cancer | No | 134 | 33.5 |
| Yes | 266 | 66.5 | |
| Total | 400 | 100 | |
| Cervical Cancer Killer Disease | No | 26 | 6.5 |
| Yes | 265 | 66.3 | |
| Do not know | 109 | 27.2 | |
| Total | 400 | 100 | |
| Cause of cervical cancer | Escherichia Coli | 87 | 21.8 |
| Human Papilloma Virus | 172 | 43.0 | |
| yeast infection | 17 | 4.3 | |
| Do not know | 124 | 31 | |
| Total | 400 | 100 | |
| Awareness of cervical cancer screening services | No | 96 | 24.0 |
| Yes | 304 | 76 | |
| Total | 400 | 100 | |
| Can Cervical Cancer be Detected | No | 60 | 15.0 |
| Yes | 340 | 85.0 | |
| Total | 400 | 100 | |
| Age to begin screening | Less than 20years | 175 | 43.8 |
| 21-40 years | 137 | 34.2 | |
| Above 41 years | 13 | 3.2 | |
| Do not know | 75 | 18.8 | |
| Total | 400 | 100 | |
| where is cervical cancer screening done | Hospital | 342 | 85.5 |
| Pharmacy | 40 | 10.0 | |
| traditional doctor | 18 | 4.5 | |
| Total | 400 | 100 | |
| can cervical cancer be treated
|
Yes | 272 | 68.0 |
| No | 23 | 5.8 | |
| Do not know | 105 | 26.2 | |
| Total | 400 | 100 |

Figure 1: Overall knowledge level of participants on cervical cancer
From figure 1, majority of the participants 64% had adequate knowledge on cervical cancer, its causes, risk factors, signs and symptoms, methods of prevention, where screening is done and the age to start screening, while 36% of the participants had poor knowledge of cervical cancer.
Participants Level Of Uptake Of Cervical Cancer Screening Service
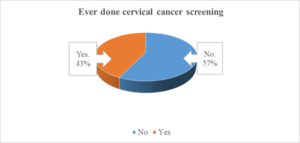
Figure 2: Distribution of participants based on uptake cervical cancer screening.
From figure 2, The level of uptake of cervical cancer screening services in this study was 43%.
Enabling Factors Of Cervical Cancer Screening
From table 4a people living in Kumba Town had 2.2 times more chances of doing cervical cancer screening compared to those living in Fiango (COR=2.15; CI:1.24-3.91, p value=0.01). Having adequate knowledge about cervical cancer increases the chances of uptake by 4.5 times (COR=4.45; CI: 2.86-7.27, p value=0.008). Positive attitude increase uptake of cervical cancer screening by 2.39 (COR= 2.39; CI: 1.41-4.40, p value= <0.000). Receiving husband encouragement reduced level of uptake of cervical cancer screening by 0.25 times (COR =0.25 CI: 0.19-0.81, p valu=0.007). Living near a health facility increased the chances of uptake of cervical cancer screening services by 2 times (COR= 2.07; CI: 1.27-3.38, p value=0.009). Workers good attitude turn to reduce the uptake of cervical cancer screening by 0.40 times (COR= 0.40; CI: 0.19-0.81, p value=0.002) less likely to do cervical cancer screening provided. Women who perceived the price of cervical cancer screening affordable were 10 times more likely of doing cervical cancer screening compared to those who did not know about the price of screening (COR= 10.21; CI: 5.96-17.48, p value=<0.000) while women who perceived the price as expensive were more than 7 times (COR= 7.45; CI: 4.18-13.32, p value=<0.000) more likely of doing screening compared to those who did not know the price. Receiving health worker’s encouragement increased uptake of cervical cancer by 5 times (COR= 5.45; CI: 3.40-8.74, value=<0.000) compared to those without health worker encouragement. Encouragement from community health workers were increase uptake of cervical cancer screening by 2.29 times (COR= 2.29; CI: 1.53-3.44, p value=<0.000) compared to those who did not receive it.
Table 4a: Bivariate analysis of the association between uptake of cervical cancer screening and socio demographic characteristics
| Ever done screening | ||||||
| Variable | Parameter | No | Yes | COR | 95% CI | P-value |
| Health Area | Pulletin | 4.3 | 5.0 | 1.84 | 0.86-3.91 | 0.11 |
| Kumba Town | 11.3 | 15.5 | 2.15 | 1.24-3.91 | 0.01 | |
| Kumba Station | 3.3 | 2.0 | 0.96 | 0.37-2.52 | 0.93 | |
| Kumba Mbeng | 22.5 | 10 | 0.96 | 0.40-1.19 | 0.19 | |
| Fiango (Ref) | 16 | 10.3 | 1 | |||
| Knowledge level | Adequate | 28.5 | 35 | 4.55 | 2.68-7.27 | <0.008 |
| Poor (Ref) | 28.7 | 7.8 | 1 | |||
| like to do screening | Yes | 41.8 | 37 | 2.39 | 1.41-4.04 | <0.000 |
| No (Ref) | 15.5 | 5.8 | 1 | |||
| Husband encouragement | Yes | 10.3 | 11.8 | 0.25 | 0.19-0.81 | 0.007 |
| No (Ref) | 24.5 | 37 | 1 | |||
| Nearby health facility | Yes | 40.3 | 35.5 | 2.07 | 1.27-3.38 | 0.009 |
| No (Ref) | 17 | 7.2 | 1 | |||
| Good attitude of staff | Yes | 7 | 3 | 0.4 | 0.19-0.81 | 0.002 |
| No (Ref) | 30 | 32.5 | 1 | |||
| Cost of screening | Affordable | 11 | 22 | 10.21 | 5.96-17.48 | <0.000 |
| expensive | 9.3 | 13.5 | 7.45 | 4.18-13.27- | <0.000 | |
| Do not know (Ref) | 37 | 7.2 | 1 | |||
| Health care worker encouragement | Yes | 26.5 | 35.7 | 5.45 | 3.40-8.74 | <0.000 |
| No (Ref) | 30.8 | 7 | 1 | |||
| Community health worker encouragement | Yes | 24.5 | 27 | 2.29 | 1.53-3.44 | <0.000 |
| No (Ref) | 32.8 | 15.7 | 1 | |||
From table 4b, having 2-3 children increases the uptake of cervical cancer screening by 3 times (COR=2.96; CI: 1.71-5.12, p value= 0.005), having relatives who did cervical cancer screening increased the uptake of cervical cancer screening by 6 times (COR= 6.16; CI: 3.98-9.54, p value=0.006). Feelings of having signs/symptoms of cervical cancer screening increase the uptake by 2 times (COR= 2.22; CI: 1.24-3.57, p value=0.01).
Table 4b: Bivariate analysis of the association between uptake of cervical cancer screening and socio-demographic characteristics
| Done screening (%) | ||||||
| Variable | Category | No | Yes | COR | CI (95%) | P value |
| Number of children | greater than 3 children | 10.2 | 6.7 | 1.62 | 0.84-3.12 | 0.411 |
| 2-3 children | 16.3 | 19.5 | 2.96 | 1.71-5.12 | 0.005 | |
| one child | 13.5 | 9.5 | 1.73 | 0.95-3.17 | 0.072 | |
| no child (Ref) | 17.3 | 7 | 1 | |||
| relative did screening | Yes | 15.5 | 29.7 | 6.16 | 3.98-9.54 | 0.002 |
| No (Ref) | 41.8 | 13 | 1 | |||
| attended community outreach program | Yes | 9.8 | 13.8 | 2.31 | 1.44-3.70 | 0.006 |
| No (Ref) | 47.5 | 29 | 1 | |||
| feelings of having signs and symptoms | Yes | 7.3 | 10 | 2.11 | 1.24-3.57 | 0.01 |
| No (Ref) | 50 | 32.7 | 1 | |||
Determinants Of Uptake Of Cervical Cancer Screening
For controlling of confounders, the following variables were included in the multivariate analysis to determine the Factors associated with the uptake of cervical cancer screening services: health area, age, knowledge level, attitude for screening, nearby health area, husband encouragement, relative who did screening, cost of screening, number of children, feelings of signs and symptoms of cervical cancer, average monthly income and attended an outreach program.
From table 6a, after the potential confounders were controlled the independent factors positively affecting the uptake of cervical cancer were women living in Pulletin Health Area (AOR =3.03, CI=1.02-8.99, p value=0.050) and Kumba Town Health Area (AOR=2.55, CI=1.20-5.44, p value=0.023), having age between 35-44 years (AOR=1.96 CI=1.03-3.71, p value=0.041), adequate knowledge (AOR=2.96, CI=1.56-5.59), having a relative who did screening (AOR 3.82, CI=2.08-7.00, p value=<0.000).
Table 6a: Independent determinants associated with uptake cervical cancer screening
| Done screening (%) | AOR | 95%CI | |||||
| Variable | Category | No | Yes | Lower | Upper | P value | |
| Health Area | Pulletin | 4.3 | 5 | 3.03 | 1.02 | 8.99 | 0.050 |
| Kumba town | 11.3 | 15.5 | 2.55 | 1.12 | 5.44 | 0.023 | |
| Kumba Station | 3.3 | 2 | 0.72 | 0.2 | 2.58 | 0.624 | |
| Kumba Mbeng | 22.5 | 10 | 0.8 | 0.39 | 1.64 | 0.546 | |
| Fiango | 16 | 10.3 | 1 | . | . | . | |
| Age | 55-65years | 4.8 | 23 | 1.56 | 0.34 | 7.18 | 0.573 |
| 45-54years | 6.1 | 6.4 | 2.76 | 0.84 | 9.09 | 0.997 | |
| 35-44years | 18.3 | 3.57 | 1.96 | 1.03 | 3.71 | 0.041 | |
| 25-34years | 70.7 | 55.6 | 1 | . | . | . | |
| Knowledge level | Adequate | 28.5 | 35 | 2.96 | 1.56 | 5.59 | 0.003 |
| Poor | 28.7 | 7.8 | 1 | . | . | . | |
| Like to do screening | Yes | 41.8 | 37 | 0.53 | 0.26 | 1.07 | 0.071 |
| No | 15.5 | 5.8 | 1 | ||||
| Nearby health facility | Yes | 10.3 | 11.8 | 1.3 | 0.88 | 1.33 | 0.82 |
| No | 24.5 | 37 | 1 | . | . | . | |
| husband encouragement | Single | 22.5 | 11.5 | 0.49 | 0.24 | 1.00 | 0.050 |
| No | 24.5 | 37 | 0.47 | 0.23 | 0.97 | 0.042 | |
| Yes | 10.3 | 11.8 | 1 | . | . | . | |
| relative did screening | Yes | 15.5 | 29.7 | 3.815 | 2.079 | 7 | 0.000* |
| No | 41.8 | 13 | 1 | . | . | . | |
From table 6b death of a love one negatively affected uptake of cervical cancer (AOR=0.31, CI=0.21-0.76, p value=0.01), not knowing the cost of cervical screening negatively affects the uptake of cervical cancer screening (AOR=0.21, CI=0.10-0.42, p value=<0.000). Having average income of greater than 150.000 had a negative effect on the uptake of cervical cancer screening (AOR=0.366, CI=0.14-0.91, p value=0.03)
Table 6b: Independent determinants associated with uptake cervical cancer screening
| ever done screening % | 95% CI | ||||||
| Variable | Category | No | Yes | AOR | Lower | Upper | P Value |
| Death of a love one | yes | 6.25 | 5.75 | 0.31 | 0.12 | 0.76 | 0.01* |
| No | 51 | 37 | 1 | . | . | . | |
| Cost of screening | don’t know | 37 | 7.2 | 0.21 | 0.1 | 0.42 | ≤0.00* |
| Expensive | 9.3 | 13.5 | 0.38 | 1.49 | 0.41 | ||
| Affordable | 11 | 22 | 1 | . | . | . | |
| Number of children | greater than 3 | 10.2 | 6.7 | 2.02 | 0.76 | 5.38 | 0.16 |
| 2-3 children | 16.3 | 19.5 | 2.65 | 1.22 | 5.74 | 0.01* | |
| one child | 13.5 | 9.5 | 2.49 | 1.1 | 5.65 | 0.03* | |
| no child | 17.3 | 7 | 1 | . | . | . | |
| Feelings of signs and symptoms | Yes | 7.3 | 10 | 2.05 | 0.97 | 4.35 | 0.06 |
| No | 50 | 32.7 | 1 | . | . | . | |
| Average monthly
Income |
Greater than 150.000 | 13 | 3.5 | 0.36 | 0.14 | 0.91 | 0.03* |
| 101.000-150.000 | 12.2 | 5 | 0.81 | 0.33 | 1.95 | 0.63 | |
| 50.000-100.000 | 25.3 | 13 | 1.55 | 0.8 | 2.99 | 0.19 | |
| less than 50.000 | 49.3 | 25 | 1 | . | . | . | |
| Attended outreach program | yes | 9.8 | 13.8 | 1.53 | 0.79 | 2.98 | 0.21 |
| No | 47.5 | 29 | 1 | . | . | . | |
DISCUSSION
This study investigated the determinants of cervical cancer screening uptake among women aged 25-65 in Kumba. The discussion is structured around the study’s objectives.
Knowledge of Participants about Cervical Cancer:
Overall knowledge of cervical cancer was adequate at 64%, contrasting with other studies reporting poor knowledge (Mbaka et al., 2018). This higher knowledge level may be attributed to effective health education by healthcare personnel and community health workers, frequent hospital visits, and accessible health facilities. This finding aligns with a study in Kumbo (Donatus et al., 2019) but differs from Simo et al. (2021), who found that most participants had never heard of cervical cancer. These differences likely stem from variations in socio-demographic characteristics and health education levels. Despite the relatively high knowledge level, some women remain unaware, highlighting the need for continued education, emphasizing risk factors, signs and symptoms, prevention methods, and screening locations.
Level of Uptake of Cervical Cancer Screening:
Cervical cancer screening uptake was low at 43%, compared to the WHO’s 70% recommendation. While this represents a promising uptake due to increased awareness, it still requires improvement. Studies suggest that poor knowledge is a major barrier to screening (Mbaka et al., 2018), emphasizing the importance of ongoing education through various channels. This study’s uptake rate is similar to studies in Southeast Ethiopia and Kumbo (Donatus et al., 2019; Gizaw et al., 2022) but higher than studies in Ambo Town, Central Uganda, and Zimbabwe (Natae et al., 2021; Isabirye et al., 2022, 2020), which attributed low uptake to poor knowledge. Conversely, it’s lower than a study in Eastern Ethiopia (Tesfaye et al., 2023), where high knowledge levels, due to awareness campaigns, led to higher uptake.
Determinants of Uptake of Cervical Cancer Screening Services:
- Health Area: Women in Kumba Town and Pulletin were more likely to be screened than those in Fiango, possibly due to proximity to screening facilities (KBH and Regional Hospital Kumba) and those health areas are in the urban settings. This aligns with studies in Southwest Ethiopia and West Ethiopia (Gizaw et al., 2022), which showed increased uptake with shorter distances to health facilities and in urban areas (Rawlence et al., 2016).
- Age: Women aged 35-44 were more likely to be screened than those aged 25-34. This may be due to symptomatic irregular bleeding experience women experience make them to perceive themselves at risk of cervical cancer. This is consistent with studies in West Ethiopia and Ambo Town (Akokuwebe et al., 2021; Gizaw et al., 2022; Natae et al., 2021), but contrasts with a study in Josua O. et al. (Okyere et al., 2021) which found higher uptake in younger women.
- Knowledge: Adequate knowledge of cervical cancer was associated with a threefold increase in screening uptake. This highlights the importance of sensitization and education by healthcare personnel and community health workers. This aligns with studies in Eastern Ethiopia, Oromia Ethiopia, and Myanmar (Nandar & Laosee, 2015; Natae et al., 2021; Tesfaye et al., 2023).
- Husband Encouragement: Lack of husband encouragement was negatively associated with screening uptake. This highlights the need for male involvement in promoting women’s health. This finding supports a study in Addis Ababa, which identified lack of husband encouragement as a barrier (Hussein et al., 2024).
- Death of a Loved One: Experiencing the death of a loved one may negatively impact screening uptake due to misconceptions about screening leading to mortality. Addressing these misconception are crucial to uptake of cervical cancer screening.
- Cost of Screening: Not knowing the price of screening was negatively associated with uptake, likely due to assumptions of high cost. Transparency about costs and highlighting the cost-effectiveness of screening are essential.
- Relatives’ Screening Status: Having relatives who had been screened was positively associated with screening uptake, suggesting the influence of social networks and shared experiences.
- Parity: Having one or two to three children was positively associated with screening uptake, possibly due to increased interaction with healthcare providers during routine visits. This aligns with a study in Oromia Ethiopia (Gizaw et al., 2022) but differs from studies in Malawi and Ambo Town (Natae et al., 2021; Tadesse et al., 2023), which showed increased uptake with more deliveries. These differences may be due to variations in research methods.
- Income: Surprisingly, higher income was negatively associated with screening uptake. This is explained by the fact that most women with higher income were in between the ages of 25-34 years making them belief they are less likely of having cervical cancer as they consider it as a disease of the old. Targeted interventions are needed for this group. This contrasts with a study in Latin America, which found a positive association between wealth and screening (77).
Study Strengths and Limitations:
Study strength; The cross-sectional design allowed assessment of various factors influencing screening uptake of cervical cancer.
Study limitation, the study could cannot establish cause and effect relationship due to its one-point-in-time nature. Recall bias and selection bias (prioritizing elderly women in a household of two women) is also a potential limitation of this study. Generalizability may be limited due to the focus on five urban health areas in Kumba. Information bias related to self-reporting is also possible.
CONCLUSION
While knowledge of cervical cancer is relatively high in Kumba, uptake of screening remains low compared to WHO targets. Continuous education about risk factors, symptoms, and screening locations is crucial. Enabling factors include living in specific health areas, being a private employee, having children, adequate knowledge, positive attitudes, proximity to facilities, perceived affordability, healthcare worker encouragement, having screened relatives, and experiencing potential symptoms. Determinants include age, parity, knowledge, marital status, and having screened relatives. Addressing misconceptions, promoting male involvement, ensuring cost transparency, and developing targeted interventions for specific groups are vital for increasing screening uptake and achieving WHO goals for cervical cancer elimination.
RECOMMENDATIONS
The government through the ministry of public health should increase the number of cervical cancer screening facilities in Kumba and reduce the price of screening, with the amount made known to the public.
Health personnel and community health workers should actively sensitize the Kumba population about cervical cancer screening using available media such as radio, television, social media and bill boards. Health facilities should periodically organize free cervical cancer screening campaigns
Screened relatives and friends should always share their experiences about the screening process to the unscreened relatives. This serve as positive reinforcers for cervical cancer screening.
List of abbreviations
| Q&A | Questions and Answers |
| AOR | Adjusted Odd Ratio |
| CI | Confidence Interval |
| COR | Crude Odd Ratio |
| DNA | Deoxyribonucleic acid |
| HPV | Human papilloma virus |
| KND | Kumba North District |
| KSD | Kumba South District |
| VIA | Visual inspection with Acetic Acid |
| VILLI | Visual inspection with Lugol’s Iodine |
Declarations
This work is original, with all used sources properly cited and referenced with genuine data collected
No conflict of interest existed in this work
Consent for publication
Not Applicable.
Availability of data and materials
The data set generated and analyzed in this study, are available from the corresponding author on reasonable request.
Competing interest
No competing interest exist among authors of this study.
Funding
Not applicable.
Author’s contributions
Not applicable.
ACKNOWLEDGEMENT
Special appreciation to all the data collectors, my colleagues in KBH, and all the participants who participate in this study.
Author’s information
Ngon Emmanuel Wasibang (MPH) Epidemiology and Biostatistics University of Buea),
Dr. Simo Wambo Andre (Obstetrician and Gynecologist, Limbe Regional Hospital, lecturer Faculty of Health Sciences University of Buea), email: asimo83@hotmail.com
Dr. Tchounzou Robert (Obstetrician and Gynecologist, Douala Gyneco Obstetric Hospital, lecturer Faculty of Health Sciences University of Buea), email: rtchounzou@gmail.com
Corresponding author
Correspondence to Ngon Emmanuel Wasibang, University of Buea Cameroon. Email; ngonemmanuelwasibang@gmail.coom phone +237676114605
REFERENCES
- Ahmed, S. A., Sabitu, K., Idris, S. H., & Ahmed, R. (2013). Knowledge, attitude and practice of cervical cancer screening among market women in Zaria, Nigeria. Nigerian Medical Journal: Journal of the Nigeria Medical Association, 54(5), 316.
- Akokuwebe, M. E., Idemudia, E. S., Lekulo, A. M., & Motlogeloa, O. W. (2021). Determinants and levels of cervical Cancer screening uptake among women of reproductive age in South Africa: Evidence from South Africa Demographic and health survey data, 2016. BMC Public Health, 21(1), 2013.
- Al-Oseely, S. A., Manaf, R. A., & Ismail, S. (2023). Barriers and Facilitators Factors to Uptake of Cervical Cancer Screening Among Women in Low-and Middle-income Countries: A Narrative Review. Malaysian Journal of Medicine & Health Sciences, 19(4).
- Arslan, H. N., & Oruc, M. A. (2022). Results from a cervical cancer screening program in Samsun, Turkey. BMC Women’s Health, 22(1), 331. https://doi.org/10.1186/s12905-022-01916-6
- Ayenew, A. A., Zewdu, B. F., & Nigussie, A. A. (2020). Uptake of cervical cancer screening service and associated factors among age-eligible women in Ethiopia: Systematic review and meta-analysis. Infectious Agents and Cancer, 15, 1–17.
- Balogun, M., Odukoya, O., Oyediran, M., & Ujomu, P. (2012). Cervical cancer awareness and preventive practices: A challenge for female urban slum dwellers in Lagos, Nigeria. African Journal of Reproductive Health, 16(1).
- Bedell, S. L., Goldstein, L. S., Goldstein, A. R., & Goldstein, A. T. (2020). Cervical cancer screening: Past, present, and future. Sexual Medicine Reviews, 8(1), 28–37.
- Bencherit, D., Kidar, R., Otmani, S., Sallam, M., Samara, K., Barqawi, H. J., & Lounis, M. (2022). Knowledge and awareness of Algerian students about cervical cancer, HPV and HPV vaccines: A cross-sectional study. Vaccines, 10(9), 1420.
- Donatus, L., Nina, F. K., Sama, D. J., Nkfusai, C. N., Bede, F., Shirinde, J., & Cumber, S. N. (2019). Assessing the uptake of cervical cancer screening among women aged 25-65 years in Kumbo West Health District, Cameroon. Pan African Medical Journal, 33(1).
- Gao, M., Hu, S., Zhao, X., You, T., Jit, M., Liu, Y., Qiao, Y., Zhao, F., & Wang, C. (2023). Health and economic impact of delaying large-scale HPV vaccination and screening implementation on cervical cancer in China: A modelling study. The Lancet Regional Health–Western Pacific, 36.
- Gizaw, A. T., El-Khatib, Z., Wolancho, W., Amdissa, D., Bamboro, S., Boltena, M. T., Appiah, S. C. Y., Asamoah, B. O., Wasihun, Y., & Tareke, K. G. (2022). Uptake of cervical cancer screening and its predictors among women of reproductive age in Gomma district, South West Ethiopia: A community-based cross-sectional study. Infectious Agents and Cancer, 17(1), 1–10.
- Harini, R., & Rosyad, A. A. (2021). Husband Support Mediates the Association between Self-Efficacy and Cervical Cancer Screening among Women in the Rural Area of Indonesia. Asia-Pacific Journal of Oncology Nursing, 8(5), 560–564.
- Hussein, K., Kokwaro, G., Wafula, F., & Kassie, G. M. (2024). Factors influencing the uptake and utilization of cervical cancer screening services among women attending public health centers in Addis Ababa, Ethiopia: Mixed methods study. BMC Women’s Health, 24(1), 3.
- Isabirye, A., Elwange, B. C., Singh, K., & De Allegri, M. (2022). Individual and community-level determinants of cervical cancer screening in Zimbabwe: A multi-level analyses of a nationwide survey. BMC Women’s Health, 22(1), 309.
- Isabirye, A., Mbonye, M. K., & Kwagala, B. (2020). Predictors of cervical cancer screening uptake in two districts of Central Uganda. PLoS One, 15(12), e0243281.
- Landis, F. C., Fai, N. Y.-B., Enow-Orock, G., Omer, N., & Marcelin, N. N. (2022). Perception on cervical cancer and enhancing strategies to screening uptake among women in Bamenda, Cameroon: A qualitative method. Journal of Public Health and Epidemiology, 14(4), 149–159.
- Mbaka, P., Waihenya, R., Oisebe, C., & Lihana, R. (2018). Factors affecting the uptake of cervical cancer screening in Mama Lucy Kibaki Hospital, Nairobi, Kenya. Cancer Research Journal, 6(3), 106–111.
- Moshi, F. V., Bago, M., Ntwenya, J., Mpondo, B., & Kibusi, S. M. (2019). Uptake of Cervical Cancer Screening Services and Its Association with Cervical Cancer Awareness and Knowledge Among Women of Reproductive Age in Dodoma, Tanzania: A Cross-Sectional Study. The East African Health Research Journal, 3(2), 105–114. https://doi.org/10.24248/EAHRJ-D-19-00006
- Muffih, T., Manjuha, F., Fai, M., Babey, M., Nulah, K., Welty, T., & Welty, E. (2018). Cervical Cancer Screening of Commercial Sex Workers in NW and SW Regions of Cameroon.
- Nandar, C. S., & Laosee, O. (2015). Determinants of cervical cancer screening among migrants in the Northern district of Yangon, Myanmar. Journal of Public Health and Development, 13(2), 17–31.
- Natae, S. F., Nigatu, D. T., Negawo, M. K., & Mengesha, W. W. (2021). Cervical cancer screening uptake and determinant factors among women in Ambo town, Western Oromia, Ethiopia: Community‐based cross‐sectional study. Cancer Medicine, 10(23), 8651–8661.
- Ndejjo, R., Mukama, T., Musabyimana, A., & Musoke, D. (2016). Uptake of cervical cancer screening and associated factors among women in rural Uganda: A cross sectional study. PloS One, 11(2), e0149696.
- Okunowo, A. A., Daramola, E. S., Soibi-Harry, A. P., Ezenwankwo, F. C., Kuku, J. O., Okunade, K. S., & Anorlu, R. I. (2018). Women’s knowledge of cervical cancer and uptake of Pap smear testing and the factors influencing it in a Nigerian tertiary hospital. Journal of Cancer Research and Practice, 5(3), 105–111.
- Okyere, J., Duodu, P. A., Aduse-Poku, L., Agbadi, P., & Nutor, J. J. (2021). Cervical cancer screening prevalence and its correlates in Cameroon: Secondary data analysis of the 2018 demographic and health surveys. BMC Public Health, 21(1), 1–8.
- Simo, R. T., Tchakounte, C. K., Kamdje, A. H. N., Sidje, L. M. G., Etet, P. F. S., & Telefo, P. B. (2021). Cervical cancer awareness and detection of precancerous lesions at two district health centres in the West Region of Cameroon. Asian Pacific Journal of Cancer Care, 6(3), 263–269.
- Soneji, S., & Fukui, N. (2013). Socioeconomic determinants of cervical cancer screening in Latin America. Revista Panamericana de Salud Pública, 33(3), 174–182.
- Tadesse, F., Megerso, A., Mohammed, E., Nigatu, D., & Bayana, E. (2023). Cervical Cancer Screening Practice Among Women: A Community Based Cross-Sectional Study Design. INQUIRY: The Journal of Health Care Organization, Provision, and Financing, 60, 00469580231159743.
- Tadzong-Awasum, G., & Morgan, J. (2021). Women’s perspectives on cervical cancer screening in Biyemassi, Yaoundé, Cameroon. International Public Health Journal, 13(2), 147–155.
- Tesfaye, D., Weldegebreal, F., Ayele, F., & Dheresa, M. (2023). Cervical cancer screening uptake and associated factors among Women Living with Human Immunodeficiency Virus in public hospitals, eastern Ethiopia. Frontiers in Oncology, 13.
- Wakwoya, E. B., Gemechu, K. S., & Dasa, T. T. (2020). Knowledge of cervical cancer and associated factors among women attending public health facilities in Eastern Ethiopia. Cancer Management and Research, 10103–10111.
- Wang, W., Arca, E., Sinha, A., Hartl, K., Houwing, N., & Kothari, S. (2022). Cervical cancer screening guidelines and screening practices in 11 countries: A systematic literature review. Preventive Medicine Reports, 28, 101813.