
From Risk to Resilience: A Comprehensive Review of Eating Disorder Prevention Strategies
- Berrak Itır Aylı
- Ayşe Tülay Bağcı Bosi
- 187-198
- Mar 3, 2025
- Public Health
From Risk to Resilience: A Comprehensive Review of Eating Disorder Prevention Strategies
Berrak Itır Aylı1*, Ayşe Tülay Bağcı Bosi2
1Graduate School of Health Sciences, Hacettepe University, Ankara, Turkey
2Institute of Public Health, Hacettepe University, Ankara, Turkey
*Corresponding Author
DOI: https://doi.org/10.51244/IJRSI.2025.121500016P
Received: 25 January 2025; Accepted: 30 January 2025; Published: 03 March 2025
ABSTRACT
Globally, the correlation between beauty ideals and thinness, further amplified by the influential presence of social media, has contributed to the increasing prevalence of eating disorders. Eating disorders, which are interrelated to preoccupations over one’s body image and body weight, give rise to a number of medical, functional, social, and mental health complications, hence presenting substantial dangers to the overall well-being of the general population. This study conducted a comprehensive assessment of more than 50 scholarly articles pertaining to the topic, with the aim of assessing the present status of eating disorders and exploring the existing initiatives in the prevention and treatment of such diseases.
Keywords: Eating disorder, anorexia, bulimia, adolescence, prevention
INTRODUCTION
During the period of adolescence, there is a notable tendency for eating disorders to emerge, resulting in substantial consequences for an individual’s physical health and mental health. Guided by the escalating incidence of eating disorders in contemporary times, there is a constantly growing amount of scholarly inquiry aimed at investigating the methods and strategies for averting, regulating, and assessing the effects and impact of said effects of eating disorders on individuals. Hudson et al. [2] reported that the prevalence of binge eating disorder (BED) surpasses that of BN or AN, and its prevalence is experiencing a more rapid increase compared to the aforementioned disorders. In Figure 1, three major eatind disorders and their symptoms are shown.
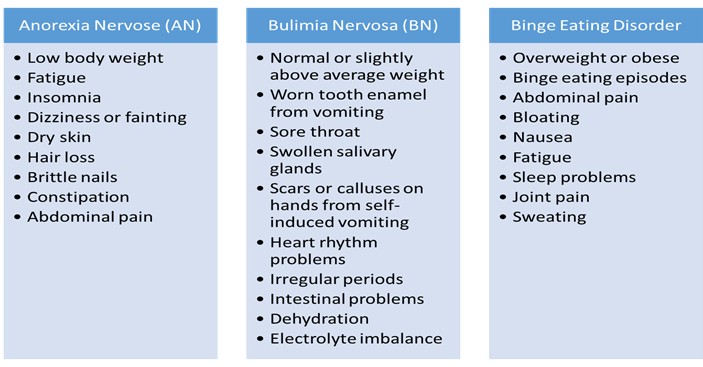
Figure 1. Common Signs of Eating Disorders
Hudson and colleagues (2010) underscored the significance of BED as a substantial concern within public health. The condition known as BED has been found to have associations with obesity, diminished quality of life, disengagement from social activities as a result of physical inactivity, and symptoms of sadness. According to Grucza (3), notable amounts of people diagnosed with BEDare reported to have a body mass index that is higher than 25, with around 70% of these individuals falling into the obese category. According to Grilo (4), it was also emphasized that a significant proportion of persons diagnosed with BED experience psychological distress, with around 74% being affected.
Eating disorders are often difficult to diagnose by the patients themselves due to shame and denial, making access to treatment challenging for this reason. According to Crow [5], less than half of patients with eating disorders seek treatment. Therefore, it is necessary not only to develop treatment methods but also to create public awareness strategies. Teaching the public that eating disorders are tangible health issues, and like any organic health problem eating disorders need to not be ignored but to be diagnosed and treated, is the first step to raising awareness. However, the public and especially the patients need also to understand that the treatments cannot be successful without a willing patient that cooperates with the treatment procedures. Developing strategies to raise awareness in public about the reality that eating disorders are like any other health problem that they are not, in fact, something to be ashamed of or denied, and that they can lead to serious consequences, even death if left unaddressed, is essential.
Watson et al. [1] have categorized prevention programs for eating disorders into different methods, including face-to-face and online interventions, as well as universal and selective interventions targeting higher-risk groups. According to the results obtained in the same study, universal approaches emerge as an approach that minimizes risk, particularly by leveraging the power of the media. In selective prevention methods, the dissonance-based approach has been identified as the most efficient method. Additionally, Watson emphasizes that eating disorders can occur at any age, highlighting the importance of addressing this issue universally rather than focusing on specific age groups. According to Arcelus et al [6], AN and BN are more prevalent, especially in girls under the age of 15, and directly impact social life. Similarly, Smink et al.[7] emphasize that eating disorders are more prevalent, especially during the preadolescent period. Herpertz-Dahlmann [8] et al. highlight that adolescent girls are more frequently faced with these disorders compared to adolescent boys. Thirteen percent of girls show symptoms of eating disorders.
In the study by Vanie et al. [9], it was noted that body dissatisfaction is significantly more common in females compared to males and females have higher self-awareness regarding this matter when compared to males. Another research group [10], in their study, reported that women engaged in sports have a higher body obsession compared to men.
The increasing use of social media, body dissatisfaction, and low self-esteem are identified by Jacobi et al. [11] as key factors contributing to the rise of such disorders. All studies indicate that eating disorders are on the rise, especially during childhood and adolescence, emphasizing the necessity to develop prevention programs tailored to this age group.
Zanelle and Lee (12) underscored the significant rise in eating disorders globally, with an increase of over 30%. Furthermore, there has been a growing probability of encountering AN and BN. The study primarily examined seven fundamental theories, specifically self-esteem theory, interpersonal theory, emotion regulation theory, executive function theory, social neuroscience theory, theory of mind, and trans-diagnostic theory. Upon thorough examination of the enormous corpus of literature pertaining to disordered eating, a number of deficiencies and limitations in the existing research were identified as seen in Table 1. The next section will focus on areas for improvement using a more comprehensive approach. By collecting the entire body of literature, potential research and intervention insights can be gained.
Table 1. Highlights and disputations in the seven theories and the major correlated variations on eating disorders [adopted by ref 12]
| Theory | Important Highlights |
| Self-esteem | The role of bidirectional mediation on disordered eating; the interpersonal motivation element; the vicious circle between low self-esteem, body dissatisfaction, and
disordered eating |
| Interpersonal | social influence; relational stress; conflict; and unfavorable interpersonal assessments; heighten the impact of social phobias on the symptoms of disordered eating |
| Emotion regulation | Overall affect, stress reactivity factor, binge eating and the behaviors that unintentionally occur to compensate and numb negative emotions, and restrictive diets to improve self-regulation |
| Executive function (EF) | Impulsiveness, decision-making process, mental flexibility/shifting capacities, global understanding, and span of attention are among the cognitive and neurobiological factors. Executive function deficiencies and poor eating behavior are ambiguously correlated. |
| Social Neuroscience | biological factors; neurological mechanisms; stimulation of particular neurological pathways during social interactions; impact on eating habits and concerns about body image |
| Theory of mind (ToM) | Perspective-taking as it relates to development; the ability to interpret the ideas, feelings, and mental states of others; Mixed findings on ToM deficiencies in people with eating disorders |
| Transdiagnostic | factors that both restricting and binge eating have in common; Mechanisms including psychological, neurological, and cognitive transdiagnostic data to explain the range of eating behaviors |
Because of the scarcity of information, the treatment of eating disorders is often perceived as a challenging process. The problem is frequently overlooked or denied. Therefore, it is necessary to develop new and innovative treatment methods, raise public awareness about this issue, and ensure access to treatment even through online platforms [13]. Within the scope of this literature review, meta-analyses related to this topic will be provided, and statistical study results will be presented. Another part of the study will present information obtained from the literature about both traditional and modern treatment methods developed in recent years with the advancement of technology
META- ANALYSIS STUDIES
In their work, Litvin et al. (2014) conducted a comprehensive review and meta-analysis of glutathione (GSH). This study also took into account comparisons between conventional face-to-face therapy and interventions with control groups. A total of 39 research, including a sample size of 3396 participants, met the inclusion criteria for the self-help/guided self-help conditions. The findings indicated that both guided and unguided self-help interventions demonstrated a statistically significant, albeit small, negative effect size in comparison to alternative therapies (n = 15; g = -0.17; 95% CI: -0.27 to -0.07, p < .01). Conversely when held in comparison with the control group, these interventions exhibited a moderately positive effect size (n = 44; g = 0.49; 95% CI: 0.37 to 0.61, p < .01).
In their research, Huey et al. (15) categorized a total of 271 female participants into three distinct groups. The groups included in this study are categorized as follows: Internet dissonance-based intervention (DBI-I), Internet cognitive-behavioral intervention (CBI-I), and no intervention (NI), using random assignment. The initial two categories of interventions involved the implementation of online sessions on a frequency of four times per week. Based on the findings, there was a notable decrease in body dissatisfaction among women who underwent both the initial and subsequent forms of treatment. The initial intervention resulted in a decrease in eating pathology as opposed to the control group that received no treatment.
Mara et al. [16] performed meta-analysis to assess the effectiveness of guided and unguided self-help treatments for eating disorders prevention and treatment in young adults that were aged between 13 and 24 years. Given that eating disorders bimodally peak between the ages of 13–14 and 17–19, it is crucial to look at young adults more broadly instead of focusing solely on teenagers. In the study, research was conducted on a group of 985 participants with an average age of around 19. After treatment, self-help intervention was found to have a very small impact although after statistical analysis this effect was found to be insignificant.
In a research conducted by Austin in the year 2000, a total of 20 distinct experimental intervention studies were analyzed. The findings of this investigation indicated that the interventions investigated did not result in any discernible increase in treatment outcomes [17]. In a study conducted by Stice (2007), contrasting the findings from seven years prior, it was ascertained that out of the prevention programs that were incorporated in the study, %51 yielded a noteworthy decrease in at least one risk factor associated with eating disorders. Additionally, 29% of the programs were successful in mitigating eating disorder-related behaviors among the participants.
In the study by Beccia et al.,[19] two meta-analyses were conducted. The first one pertains to mindfulness-based interventions versus control and their short-term effects post-treatment, while the second one focuses on control-based mindfulness interventions and their long-term effects. The findings of this review imply that specific mindfulness-based programs that involve meditation may decrease eating disorder risk factors and increase protective variables, albeit conclusions can only be reached from a limited volume and quality of research. Given these findings, more study is required to determine the most effective way to carry out such interventions and the influence of mindfulness on these results.
The study administered by Shaw et al. (2020) aims to examine a potential relationship between baseline eating disorder risk factors and symptoms and sexual orientation, specifically categorizing individuals as either heterosexual or sexual minority. Additionally, the study investigates whether the effects of interventions are moderated by dissonance-based Body Project variants, as well as the association between baseline risk factors and changes in future eating disorder symptoms. A total of 680 women with body shape dissatisfaction were subjected to random assignment, wherein they were allocated to one of three groups: the Body Project, the eBody Project, or a control group that viewed educational videos. Subsequently, the participants proceeded to fill out questionnaires pertaining to risk variables and symptoms associated with eating disorders during the pretest, posttest, and follow-up assessments conducted at six, twelve, twenty-four, and thirty-six months. The findings of the study showed that women who identify as sexual minorities exhibited elevated levels of sad mood and reduced psychosocial functioning at the beginning of the study. However, there were no discernible disparities in other characteristics associated with the emergence of eating disorders or the manifestation of related symptoms.
In light of the reviewed studies, several key limitations can be identified:
- The majority of the studies were conducted with female participants, limiting their ability to represent the broader population.
- Similarly, another constraint is that most studies focused on adolescents and young adults, making their findings applicable only to specific age groups. Consequently, older individuals and those from diverse socioeconomic backgrounds remain underrepresented.
- Given that the results primarily examine a specific demographic, the generalizability of the findings is restricted.
- From a methodological perspective, some studies rely solely on self-report measures, with limited use of more objective assessment techniques.
- Another notable limitation is the short follow-up periods in certain studies, which makes it difficult to assess the long-term effects of the interventions.
PREVENTION METHODS
Eating disorders pose a substantial challenge within the domain of public health. Based on data derived from a nationally representative sample [21], the estimated lifetime prevalence rates of diverse eating disorder diagnoses, including AN, BN, binge eating disorder, and other particular feeding or eating disorders, are reported to be 4.95% among women and 2.24% among men. Furthermore, it is worth noting that empirical evidence obtained from population surveys suggests that around 12.5% of adolescent and young adult females residing in the United States exhibit eating pathology. This encompasses a spectrum of disorders including threshold, subthreshold, and atypical eating disorders [22].
Numerous therapy modalities have been devised due to these rationales. In their 2004 study, Stice and Shaw [23-25] categorized preventative programs into three distinct groups: general psychoeducational programs, media literacy programs, and selectively delivered interactive programs that specifically address psychological and behavioral risk factors. In the aforementioned study, it was determined that the aforementioned programs exhibited a level of effectiveness amounting to 51%. This section presents a comprehensive overview of the treatment and preventative strategies highlighted in many scholarly investigations.
Guided Self Help (GSH)
One of the treatment methods is the guided self-help (GSH) approach. Banasiak et al. [26] provide GSH as a primary care service in their study. The study investigated the GSH process guided by general practitioners and its effects within 3-6 months. According to the results, the GSH method demonstrated faster improvement compared to the DTC method.
Physiological Therapy (PT)
According to Bower et al [27], the current demand for psychological therapy cannot be satisfied by traditional forms of delivery. Alternative delivery methods including short-term therapies, group therapy, and self-help may be beneficial. Delivering alternate types of therapy using a tiered care model has considerable potential to boost the effectiveness of therapy and guarantee positive patient outcomes.
One of the methods that can be considered among psychological treatment approaches was proposed by Sigall and Pabst [28]. Providing education in schools to counteract body-based intolerance and increase students’ awareness in this regard is a method that can prevent eating disorders. Particularly, it has been commented that understanding and learning the connections regarding how the body is utilized could be beneficial for both staff and students.
Cognitive Behavioral Therapy (CBT)
Carter and Fairburn (1998) recommended cognitive-behavioral therapy (CBT) as a potentially efficacious treatment modality for patients diagnosed with BED. According to the aforementioned study, CBT is found to have a significant impact in mitigating related symptoms, including concerns related to body weight and self-esteem problems that are exacerbated by one’s perception of their body.
The results of the online-guided self-help program for BN, which was carried out in four European countries as a component of the SALUT European research project, have proved that symptoms of eating disorders decrease in patients who take part in the programs. The fact that the same decrease in symptoms was seen in all four of the countries that were involved in this study also shows the importance of the programs in helping patients and further validates the results [30].
Carrard et al [31] performed a randomized study with control groups to examine the effectiveness of Online self-help treatment for BED that is based on CBT. According to their results, this method improved important aspects of the sickness. It served as many participants’ initial eating disorder treatment they wouldn’t have known where to look for assistance without the visibility that the Internet offers. Some individuals who still required assistance after the online intervention were more eager to speak with a clinician. These factors allow for the recommendation of an Internet self-help program as a first line of BED treatment.
Fichter et al. [32,33] conducted an investigation on the CBT-based prevention program for patients currently diagnosed, treated, and discharged with AN. The program was associated with small improvements in clinician-rated BN and global eating disorder psychopathology at the end of the intervention.
Media Literacy
Programs such as Life Smart and MABIC-Project have been proven to be effective in preventing the emergence of eating disorders in both children and teenagers. In these programs that use an interactive approach, the worst-case scenarios that an individual might face in the case of an eating disorder are emphasized, and protective behaviors are attempted to be instilled. Similarly, the World Health Organization (WHO) also stressed the essential role of life skills education in avoiding psychosocial health problems in 1997. Utilizing the power of media at this point is an extremely effective approach [34,35].
The Project EAT (Eating Among Teens) model, emphasizes that regular family meals, where the family sits down together, are a particularly protective model for girls. This model contains significant findings suggesting that these meals can reduce the risks of eating disorders for girls and have a positive impact. Therefore, situations where family meals are regularly held and take place in a positive atmosphere are recommended as an effective strategy for preventing eating disorders [36].
Mindfulness-based interventions
Programs based on mindfulness practices have significantly increased in the last decade. The mentioned term ‘mindfulness’ carries the meaning of focusing on the present moment. Moreover, it aims to break the taboo of feeling weak created in the mind, based on mental development. In other words, enhancing the mind’s influence on the body actually forms the basis of mindfulness practices. For instance, areas like yoga, pilates, and hypnosis techniques involve mindfulness practices [37].
In their study conducted in 2014, Goyal et al. [38] argued that with the increasing prevalence of mindfulness practices, negative effects created in the mind could be reduced, and the focus on body image impact could be diminished. Many studies supporting Croll et al.’s [39] findings have been conducted in this regard. In their study, Coral et al. [39] argued that mindfulness education conducted during childhood serves as a protective measure against eating disorders
Internet-Based Interventions
The utilization of information and communication technologies has grown more widespread in the treatment of eating disorders, as a result of technological advancements. These interventions have the potential to prevent and raise awareness about eating disorders through fostering psychological awareness. The impact of technology-driven educational interventions on public health remains an area of ongoing investigation, with a very small body of research currently available. The research conducted by Bauer et al. [40] presents an introduction to ProYouth, an internet-based eating disorder prevention program implemented in Europe. Despite the limitations of the acquired data, they demonstrate a remarkable level of potential.
Student Bodies, the first internet-based program, is a diagnostic, treatment, and prevention program for eating disorders [41]. The program involves creating discussion groups, which are guided by a professional moderator. Observations conducted after participants worked through the educational modules for eight weeks showed a significant decrease in concerns about gaining weight, especially among at-risk participants. In 2006, a study was conducted on 480 female college students as part of the same program [42]. Following additional mediator analyses, it was seen that the online program effectively decreased the emergence of clinical and sub-clinical symptoms of disorders of eating among partakers who were either obese or reported to show compensatory behaviors at the beginning of the study.
The National Institute for Health and Care Excellence (NICE), which is based in the United Kingdom, has undertaken assessments about the efficacy of online therapeutic approaches [43]. The findings are presented in line with the guidelines that are made clear in the Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Cognitive Dissonance-Based Interventions
The Cognitive Dissonance program was developed by Eric Stice [44] and its main purpose is to break the perception of thinness as perfection, especially among young women. The study was conducted with three groups and aimed to create the perception that beauty is not parallel to thinness. In this context, the groups engaged in information exchange and idea sharing to discuss what benefits they could provide to each other [44].
The Cognitive Disease program’s societal Power Domain empowers participants by actively promoting a critical viewpoint toward societal structures (such as financial organizations), criticizing these institutions rather than people’s bodies. Additionally, participants work together to establish alternative peer norms for appropriate dialogues that reject resistant dialogues and endorse resistant self-talk through in-depth conversations and role-playing with peers (e.g., undergraduate and graduate facilitators) [45].
In a recent study conducted by Stice et al. (46), it was discovered that interventions based on cognitive dissonance resulted in noteworthy decreases in risk factors and symptoms associated with eating disorders. These risk factors and symptoms encompassed dissatisfaction with one’s body, internalization of the thin ideal, negative emotions, and engagement in dieting. The observed reductions were found to be significantly greater when compared to control conditions and alternative prevention strategies. Furthermore, Amaral and Ferreira [47,48] conducted a study that demonstrated the beneficial impact of the Body Project in promoting a positive body image, namely by enhancing individuals’ ability to value and appreciate their own bodies. The observed outcome can be ascribed to the wide range of activities in which participants were involved during the Body Project intervention. These activities effectively diminished their inclination towards the thin ideal and fostered a heightened level of body acceptance.
Rebel [49] , another cognitive dissonance-based program, is an active engagement program developed to create social solidarity, challenge societal perceptions, and eradicate the perception that psychological vulnerability is beauty. The initial results of the study suggest positive changes in self-esteem; however, they did not yield a statistically significant outcome. In another study, the same researcher [50], explored whether participants could increase their sense of empowerment and reduce the risk of eating disorders with an enhanced version of the program. The program, conducted based on the students’ voluntary participation, revealed that the participating students’ misconceptions about thinness were dispelled, and they gained an understanding of the risks associated with eating disorders.
It has been demonstrated by Becker et al. [51-53] that disordered eating prevention programs based on CDB are successful in reducing levels of body dissatisfaction, disordered eating, and risk factors for eating disorders.
Discussion About Prevention Programs
On the other hand, only a few studies have looked into the variables that can affect how well eating disorder and obesity prevention programs work. These elements might influence the intervention’s improvement and inclusion criteria. Stice et al [54] looked at variables that would mitigate the impact of Project Health, which includes cognitive dissonance exercises, and the Healthy Weight eating disorder/obesity prevention program, which promotes gradual healthy adjustments. Pretest, posttest, and 6-, 12-, and 24-month follow-up evaluations were done by college students (N = 364, 72% female) who were randomly assigned to either these interventions or the instructional video condition and who were at risk for both outcomes due to weight issues. When compared to video checks, Healthy Weight and Project Health dramatically reduced the symptoms of eating disorders in people who had higher levels of negative affect, emotional eating, and dietary fat/sugar intake.
Despite the extensive presence of preventive method studies in the literature and the research conducted by many scholars on various methods, obtaining definitive information about the effectiveness of methods is challenging. Völker et al. [55] argued that mediator analyses are necessary for this purpose. Mediators refer to changes or events that occur during the ongoing intervention after the starting point and before the outcome assessment. Information about mediators is essential to identify effective and ineffective parts of interventions, aiming to optimize the therapeutic and economic aspects of interventions.
In the study by Depa et al [56], in a study employing numerous subscales of the Food Choice Questionnaire (FCQ) that measure different motivations for food choice, after adjusting for weight management motivations, a significant association between health motivations for food choice and TOS ON was not detected. This shows that the drive to eat nutritious foods in ON is predominantly characterized by weight worries.
In 2017, Hilbert [57] did a comprehensive analysis comparing the existing guidelines for the diagnosis and treatment of eating disorders. This study revealed notable variations and contradictions within the guidelines. In a study conducted in 2018, Zeeck et al.[58] posited that adolescents exhibited a higher susceptibility to weight gain in comparison to adults. Conversely, a subsequent meta-analysis conducted by Murray et al. [59] in 2019 revealed no discernible disparities between adolescents and adults in this regard. Solmi et al. (2021) [60] suggested that the reliability of guidelines cannot be deemed absolute. The aforementioned literary works serve to underscore the ongoing significance of this subject matter, necessitating additional scholarly inquiry, given its inherent paradoxical nature.
CASE STUDIES AND REAL-WORLD EXAMPLES
Viljoen et al. investigated the application of Integrated Enhanced Cognitive Behavioural Therapy (I-CBTE) for a patient with severe and longstanding anorexia nervosa, accompanied by multiple comorbidities, including organic hallucinosis, complex post-traumatic stress disorder (CPTSD), and severe self-harm. The patient was diagnosed with anorexia nervosa following a traumatic brain injury in 2000. Despite the administration of various psychotropic medications, standard treatments remained ineffective for 17 years.In this study, the I-CBTE model was specifically implemented for this patient. The treatment process consisted of 13 weeks of inpatient care, followed by 7 weeks of stabilization and up to 40 weeks of outpatient care. Key innovations included the introduction of MDT admission planning meetings. This preparatory process aimed to enhance patients’ sense of control and autonomy, fostering therapeutic alliance and trust prior to admission, which is critical for successful engagement and treatment outcomes. Additionally, the approach improved the rate of weight restoration to 1–1.5 kg per week [61]. In the study by Khairani et al [62]., the outpatient treatment approach for an adolescent diagnosed with moderate anorexia nervosa was examined. The diagnosis was established based on the fulfillment of four specific criteria. The patient’s treatment was managed in an outpatient clinic by a multidisciplinary team, including a dietitian, psychologist, and child psychiatrist. The treatment process was structured around four key principles: (i) weight restoration, (ii) psychological intervention, (iii) pharmacological treatment when necessary, and (iv) long-term follow-up to prevent relapse. Psychological interventions included supportive therapy, behavioral interventions, assessment of the patient’s insight, enhancement of motivation for recovery, and resolution of family conflicts. The treatment was successfully implemented without the need for pharmacological intervention. In their study, Marcolini et al. [63] focus on 14 patients from the Eating Disorders Outpatients Unit at Maggiore Hospital in Bologna, who were either currently receiving treatment or had been previously treated between January 2012 and May 2023. The study examines the effects of the disorder, treatment adherence, and identifies variables that help understand the complexity of the condition. A key finding from the study is that the ego-syntonic nature of the illness often makes patients reluctant to seek treatment, while the healthcare system struggles to recognize the issue at early stages. Additionally, the presence of occupational and social dysfunctions further contributes to the chronicity of the disorder.
Lis et al. [64] conducted a case study aimed at demonstrating how a newly developed tool for assessing attachment patterns could be useful in a multimethod personality assessment and treatment plan. As a result of the study, they argue that attachment is not only a categorical classification but also a dynamic tool that can provide information about personality functioning.
In the studies by Davies and Tchanturia [65], the aim was to demonstrate how cognitive remediation therapy (CRT) can be used as part of the treatment for anorexia nervosa (AN) when other therapies, such as cognitive behavioral therapy (CBT), are too complex and intense for the patient to engage in. The purpose was to stimulate mental activities and improve thinking skills and information-processing systems. Their results showed a significant improvement in cognitive set-shifting skills after 10 sessions of CRT.
CONCLUSION
In this article, it is asserted that the association of global beauty standards with thinness triggers eating disorders, particularly when social media plays an active role. It has been emphasized that eating disorders associated with shape and weight concerns pose significant risks to the public’s physical, functional, social, and mental health. This study examined the current state of eating disorders and delved deeply into eating disorder prevention and treatment efforts by reviewing more than 50 articles on the subject.
It has been stated that eating disorders become particularly apparent during adolescence and that this period has a substantial impact on the physical and mental health of individuals. It has been stated that extensive research has been conducted on the prevention, treatment, and effects of eating disorders in recent years due to the rising prevalence of these conditions.
Studies have categorized eating disorder prevention programs using various methods, including universal and selective measures, and emphasized the effectiveness of these programs. In addition, cognitive dissonance-based interventions have been shown to substantially reduce the risk factors and symptoms of eating disorders and to be particularly effective in individuals with negative mood, emotional eating, and high levels of dietary fat/sugar intake.
Consequently, it appears that various methods are effective for preventing and treating eating disorders and that these methods have positive effects on certain risk factors and symptoms. However, it has been emphasized that studies in this area require additional research and analysis and that for the effective prevention and treatment of eating disorders, more knowledge and understanding are necessary. The purpose of this article is to cast light on future research into the prevention and treatment of eating disorders.
One of the significant findings of the study is the actionable policy recommendations for improving public health in resource-limited settings. In these settings with limited resources, it is essential to use existing resources effectively for health interventions to be successful. This necessitates increasing the cost-effectiveness of preventive health programs and reaching wider target audiences. Community-based interventions play a critical role in contributing to public health and can yield effective results by raising community awareness. Digital health applications, on the other hand, can increase access to health services in resource-constrained regions and offer low-cost solutions. Health services offered over the internet and mobile platforms can reach broader populations by increasing accessibility. Additionally, improving public health literacy can greatly enhance the effectiveness of health policies, particularly in such environments. Individuals and communities can be made aware of healthy living habits and disease prevention through educational programs. Finally, early detection and intervention of health problems are of great importance. Early intervention can prevent problems from escalating and avoid larger health expenditures in the long run.
| Ethical Approval: As it is a review article, there is no need for ethical approval.
Conflict of Interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Financial Disclosure: Authors declared no financial support |
REFERENCES
- Watson, H. J., Joyce, T., French, E., Willan, V., Kane, R. T., Tanner-Smith, E. E., McCormack, J., Dawkins, H., Hoiles, K. J., & Egan, S. J. (2016). Prevention of eating disorders: A systematic review of randomized, controlled trials. International Journal of Eating Disorders, 49(9), 833–862. https://doi.org/10.1002/eat.22577
- Hudson, J. I., Hiripi, E., Pope, H. G., Jr., & Kessler, R. C. (2007). The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biological Psychiatry, 61(3), 348–358.
- Grucza, R. A., Przybeck, T. R., & Cloninger, C. R. (2007). Prevalence and correlates of BED in a community sample. Comprehensive Psychiatry, 48(2), 124–131.
- Grilo, C. M., & Masheb, R. M. (2005). A randomized controlled comparison of guided self-help cognitive behavioral therapy and behavioral weight loss for binge eating disorder. Behavior Research and Therapy, 43(11), 1509–1525.
- Crow, S. J., Peterson, C. B., Levine, A. S., Thuras, P., & Mitchell, J. E. (2004). A survey of binge eating and obesity treatment practices among primary care providers. International Journal of Eating Disorders, 35(3), 348–353.
- Arcelus, J., Mitchell, A. J., Wales, J., & Nielsen, S. (2011). Mortality rates in patients with AN and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry, 68, 724–731.
- Smink, F. R., van Hoeken, D., & Hoek, H. W. (2012). Epidemiology of eating disorders: Incidence, prevalence, and mortality rates. Current Psychiatry Reports, 14, 406–414.
- Herpertz-Dahlmann, B., Wille, N., Holling, H., Vloet, T. D., Ravens-Sieberer, U., & Group, B. S. (2008). Disordered eating behavior and attitudes, associated psychopathology and health-related quality of life: Results of the BELLA study. Eur Child Adolesc Psychiatry, 17 Suppl 1, 82–91.
- Vani, M. F., Pila, E., Willson, E., & Sabiston, C. M. (2020). Body-related embarrassment: The overlooked self-conscious emotion. Body Image, 32, 14–23.
- Soulliard, Z. A., Kauffman, A. A., Fitterman-Harris, H. F., Perry, J. E., & Ross, M. J. (2019). Examining positive body image, sport confidence, flow state, and subjective performance among student athletes and non-athletes. Body Image, 28, 93–100. https://doi.org/10.1016/j.bodyim.2018.12.009
- Jacobi, C., Fittig, E., Bryson, S. W., Wilfley, D., Kraemer, H. C., Taylor, C. B. (2011). Who is really at risk? Identifying risk factors for subthreshold and full syndrome eating disorders in a high-risk sample. Psychol. Med., 41, 1939–1949.
- Zanella, E., Lee, E. (2022). Integrative review on psychological and social risk and prevention factors of eating disorders including AN and BN: Seven major theories. Heliyon, 8, 1422.
- Lluch, A. (1995). Identification des conduites alimentaires par approches nutritionnelles et psychométriques: Implications thérapeutiques et préventives dans l’obésité humaine. Thesis, Université Henri Poincaré, Nancy.
- Litvin, S., Saunders, R., Jefferies, P., Seely, H., Pössel, P., Lüttke, S. (2023). The Impact of a Gamified Mobile Mental Health App (eQuoo) on Resilience and Mental Health in a Student Population: Large-Scale Randomized Controlled Trial. JMIR Mental Health, 10, e47285. https://doi.org/10.2196/47285
- Huey, S. J., Park, A. L., Galán, C. A., Wang, C. X. (2023). Culturally Responsive Cognitive Behavioral Therapy for Ethnically Diverse Populations. Annual Review of Clinical Psychology, 19, 51–78. https://doi.org/10.1146/annurev-clinpsy-080921-072750
- Mara, M., Greene, D., Watson, H., Shafran, R., Kenworthy, I., Creswell, C., & Egan, S. J. (2023). The efficacy of randomized controlled trials of guided and unguided self-help interventions for the prevention and treatment of eating disorders in young people: A systematic review and preliminary meta-analysis. Journal of Behavior Therapy and Experimental Psychiatry, 78, 101777.
- Austin, S. B. (2000). Prevention research in eating disorders: Theory and new directions. Psychol. Med., 30, 1249–1262.
- Stice, E. (2001). A prospective test of the dual-pathway model of bulimic pathology: Mediating effects of dieting and negative affect. J. Abnorm. Psychol., 110, 124–135.
- Beccia, A., Dunlap, C., Hanes, D., Courneene, B., & Zwickey, H. (2018). Mindfulness-based eating disorder prevention programs: A systematic review and meta-analysis. Mental Health & Prevention, 9, 1–12.
- Shaw, H., Rohde, P., Desjardins, C. D., & Stice, E. (2020). Sexual orientation correlates with baseline characteristics but shows no moderating effects of dissonance-based eating disorder prevention programs for women. Body Image, 32, 94–102.
- Duncan, A. E., Ziobrowski, H. N., & Nicol, G. (2017). The prevalence of past 12-month and lifetime DSM-IV eating disorders by BMI category in US men and women. European Eating Disorders Review, 25(3), 165–171.
- Stice, E., Gau, J. M., Rohde, P., & Shaw, H. (2017). Risk factors that predict future onset of each DSM–5 eating disorder: Predictive specificity in high-risk adolescent females. Journal of Abnormal Psychology, 126(1), 38–51.
- Stice, E., & Shaw, H. (2004). Eating disorder prevention programs: A meta-analytic review. Psychological Bulletin, 130(2), 206–227.
- Stice, E., Shaw, H., Black Becker, C., & Rohde, P. (2008). Dissonance-based interventions for the prevention of eating disorders: Using persuasion principles to promote health. Prevention Science, 9, 114–128.
- Stice, E., Shaw, H., & Marti, C. N. (2007). A meta-analytic review of eating disorder prevention programs: Encouraging findings. Annual Review of Clinical Psychology, 3, 207–231.
- Banasıak, S., Paxton, S., & Hay, P. (2005). Guided self-help for BN in primary care: A randomized controlled trial. Psychological Medicine, 35(9), 1283–1294. https://doi.org/10.1017/S0033291705004769
- Bower, P., & Gilbody, S. (2005). Stepped care in psychological therapies: Access, effectiveness and efficiency: Narrative literature review. The British Journal of Psychiatry, 186(1), 11–17. https://doi.org/10.1192/bjp.186.1.1
- Sigall, B. A., & Pabst, M. S. (2005). Gender literacy: Enhancing female self-concept and contributing to the prevention of body dissatisfaction and eating disorders. Social Science Information, 44, 85–111. https://doi.org/10.1177/0539018405050462
- Carter, J. C., & Fairburn, C. G. (1998). Cognitive-behavioral self-help for binge eating disorder: A controlled effectiveness study. Journal of Consulting and Clinical Psychology, 66(4), 616–623.
- Carrard, I., Rouget, P., Fernandez-Aranda, F., Volkart, A. C., Damoiseau, M., & Lam, T. (2006). Evaluation and deployment of evidence-based patient self-management support program for BN. Behavior Research and Therapy, 44, 99–110. https://doi.org/10.1016/j.brat.2004.08.004
- Carrardi, I., Crepin, C., Rouget, P., Lam, T., Golay, A., Linderi, M.V. (2011). Randomised controlled trial of a guided self-help treatment on the Internet for binge eating disorder. Behaviour Research and Therapy, 49, 482-489.
- Fichter, M. M., Quadflieg, N., & Lindner, S. (2013). Internet-based relapse prevention for AN: Nine-month follow-up. Journal of Eating Disorders, 1, 23.
- Fichter, M. M., Quadflieg, N., Nisslmüller, K., Lindner, S., Osen, B., Huber, T., et al. (2012). Does internet-based prevention reduce the risk of relapse for AN? Behaviour Research and Therapy, 50, 180-190.
- Sanchez-Carracedo, D., Fauquet, J., Lopez-Guimera, G., Leiva, D., Punti, J., Trepat, E., Pamias, M., Palao, D. (2016). The MABIC project: An effectiveness trial for reducing risk factors for eating disorders. Behaviour Research and Therapy, 77, 23-33.
- Wilksch, S. M. (2017). How can we improve dissemination of universal eating disorder risk reduction programs? Eating Behaviors, 25, 58-61.
- Smolak, L., & Piran, N. (2012). Gender and the prevention of eating disorders. In G. McVey, M. P. Levine, N. Piran, & H. B. Ferguson (Eds.), Preventing eating-related and weight-related disorders: Collaborative research, advocacy, and policy change (pp. 201-224). Waterloo, ON: Wilfred Laurier Press.
- Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., & Devins, G. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230-241.
- Goyal, M., Singh, S., Sibinga, E. M. S., Gould, N. F., Rowland-Seymour, A., Sharma, R., & Haythornthwaite, J. A. (2014). Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Internal Medicine, 174(3), 357-368.
- Croll, J., Neumark-Sztainer, D., Story, M., & Ireland, M. (2002). Prevalence and risk and protective factors related to disordered eating behaviors among adolescents: Relationship to gender and ethnicity. Journal of Adolescent Health, 31(2), 166-175.
- Bauer, S., Papezova, H., Chereches, R., Caselli, G., McLoughlin, O., Szumska, I., Furth, E., Ozer, F., Moessner, M. (2013). Mental Health Prevention, 1, 26-32.
- Zabinski, M. F., Wilfley, D. E., Calfas, K. J., Winzelberg, A. J., & Taylor, C. B. (2004). An interactive psychoeducational intervention for women at risk of developing an eating disorder. Journal of Consulting and Clinical Psychology, 72, 914-919.
- Taylor, C. B., Bryson, S., Luce, K. H., Cunning, D., Celio Doyle, A., & Abascal, L. B., et al. (2006). Prevention of eating disorders in at-risk college-age women. Archives of General Psychiatry, 63, 881-888.
- Aardoom, J. J., Dingemans, A. E., Spinhoven, P., & Van Furth, E. F. (2013). Treating eating disorders over the internet: A systematic review and future research directions. International Journal of Eating Disorders, 46, 539-552.
- Stice, E., Shaw, H., & Marti, C. N. (2007). A meta-analytic review of eating disorder prevention programs: Encouraging findings. Annual Review of Clinical Psychology, 3, 207-231. https://doi.org/10.1146/annurev.clinpsy.3.022806.091447
- Piran, N. (2015). New possibilities in the prevention of eating disorders: The introduction of positive body image measures. Body Image, 14, 146-150.
- Stice, E., Marti, C. N., Spoor, S., & Shaw, H. (2008). Dissonance and healthy weight eating disorder prevention programs: Long-term effects from a randomized efficacy trial. Journal of Consulting and Clinical Psychology, 76(2), 329-340. https://doi.org/10.1037/0022-006X.76.2.329
- Amaral, A. C. S. (2015). Imagem corporal de adolescentes: Descrição e intervenção preventiva em âmbito escolar (Doctoral thesis). Retrieved from Universidade Federal de Juiz de Fora: https://repositorio.ufjf.br/jspui/handle/ufjf/1544
- Ferrari, E., Silva, D., & Petroski, E. (2012). Association between perception of body image and stages of behavioral changes among physical education university students. Revista Brasileira de Cineantropometria e Desempenho Humano, 14(5), 535-544. https://doi.org/10.5007/1980-0037.2012v14n5p535
- Breithaupt, L., Eickman, L., Byrne, C., & Fischer, S. (2016). REbeL peer education: A model of a voluntary, after-school program for eating disorder prevention. Eating Behaviors (current issue).
- Breithaupt, L., Eickman, L., Byrne, C., & Fischer, S. (2017). Enhancing empowerment in eating disorder prevention: Another examination of the REbeL peer education model. Eating Behaviors, 25, 38-41.
- Stice, E., Shaw, H., Becker, C. B., & Rohde, P. (2008). Dissonance-based interventions for the prevention of eating disorders: Using persuasion principles to promote health. Prevention Science, 9(2), 114-128.
- Becker, C. B., Ciao, A. C., & Smith, L. M. (2008). Moving from efficacy to effectiveness in eating disorders prevention: The sorority body image program. Cognitive and Behavioral Practice, 15(1), 18-27.
- Becker, C. B., Smith, L. M., & Ciao, A. C. (2006). Peer-facilitated eating disorder prevention: A randomized effectiveness trial of cognitive dissonance and media advocacy. Journal of Counseling Psychology, 53(4), 550-555.
- Stice, E., Desjardins, C., & Rohde, P. (2019). Moderators of two dual eating disorder and obesity prevention programs. Behaviour Research and Therapy, 118, 77-86.
- Völker, U., Jacobi, C., Trockel, M., & Taylor, B. (2014). Moderators and mediators of outcome in Internet-based indicated prevention programs. Behaviour Research and Therapy, 63, 114-121.
- Depa, J., Barrada, J. R., & Roncero, M. (2019). Are the motives for food choices different in orthorexia nervosa and healthy orthorexia? Nutrients, 3(11).
- Hilbert, A., Petroff, D., Herpertz, S., Pietrowsky, R., Tuschen-Caffier, B., Vocks, S., Schmidt, R. (2019). Meta-analysis of the efficacy of psychological and medical treatments for binge-eating disorder. Journal of Consulting and Clinical Psychology, 87. https://doi.org/10.1037/ccp0000358
- Zeeck, A., Herpertz-Dahlmann, B., Friederich, H. C., Brockmeyer, T., Resmark, G., Hagenah, U., Ehrlich, S., Cuntz, U., Zipfel, S., Hartmann, A. (2018). Psychotherapeutic treatment for anorexia nervosa: A systematic review and network meta-analysis. Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2018.00158
- Murray, S. B., Quintana, D. S., Loeb, K. L., Griffiths, S., Le Grange, D. (2019). Treatment outcomes for anorexia nervosa: A systematic review and meta-analysis of randomized controlled trials. Psychological Medicine. https://doi.org/10.1017/S0033291718002088
- Solmi, M., Radua, J., Olivola, M., Croce, E., Soardo, L., Salazar de Pablo, G., Shin, I., Kirkbride, J., Jones, J.B., Kim, P., Kim, J.H., Carvalho, J.Y., Seeman, A.F., Correll, M.V., Fusar-Poli, P., 2021. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Molecular Psychiatry. https://doi.org/10.1038/s41380-021-01161-7.
- Vilijoen, D., Ayton, A., Roberts, L., Twitchell, M., Collins, L., 2024. Applying integrated enhanced cognitive behaviour therapy (I-CBTE) to severe and longstanding eating disorders (SEED) Paper 2: An in-depth case study for clinicians. Journal of Eating Disorders, 12:172.
- Khairani, O., Majmin, S.H., Saharuddin, A., Loh, S.F., Azimah, N.M., Tohid, H., 2011. An adolescent with anorexia nervosa – A case report. Malaysian Family Physician, 6(2-3), 79-81.
- Marcolini, F., Ravaglia, A., Valenta, S.T., Bosco, G., Marconi, G., Sanna, F., Zilli, G., Magrini, E., Picone, F., Ronchi, D., Atti, A.R., 2023. Severe-enduring anorexia nervosa (SE-AN): A case series. Journal of Eating Disorders, 11:208.
- Lis, A., Mazzeschi, C., Di Riso, D., Salcuni, S., 2011. Attachment, assessment, and psychological intervention: A case study of anorexia. Journal of Personality Assessment, 93(5), 434-444.
- Davies, H., Tchanturia, K., 2005. Cognitive remediation therapy as an intervention for acute anorexia nervosa: A case report. European Eating Disorders Review, 13, 311-316.