
A Critical Review of ‘Regional Variation in Suicide Rates in Sri Lanka Between 1955 and 2011: A Spatial and Temporal Analysis’
- W.M.M. K. Weerasinghe
- K.A.A.N. Thilakarathna
- M.W.A.D.N.Wijesuriya
- 984-989
- Dec 9, 2023
- Sociology
A Critical Review of ‘Regional Variation in Suicide Rates in Sri Lanka Between 1955 and 2011: A Spatial and Temporal Analysis’
W.M.C.P. Godage, K. A. A. N. Thilakarathna,
Institute of Human Resource Advancement, University of Colombo
Faculty of Law, University of Colombo
DOI: https://dx.doi.org/10.47772/IJRISS.2023.7011077
Received: 24 November 2023; Revised: 01 December 2023; Accepted: 06 December 2023; Published: 09 December 2023
INTRODUCTION
This paper hopes to review the article written by D.W. Knipe and et all (Knipe, Padmana than, Muthuwatta, Metcalfe & Gunnell, 2017) on ‘Regional variation in suicide rates in Sri Lanka between 1955 and 2011: a spatial and temporal analysis’ which discusses about the fluctuations in suicide rates in Sri Lanka between the years of 1955-2011. The article is written using both qualitative and quantitative methods and it puts emphasis on the co-relationship between the ease of access to pesticides and suicide rates. It uses secondary data to analyze and evaluate the suicide rates of the country with the intent of finding out the relationship between the ease of access to pesticides and its effects on the suicide rate in the country. The 1960s and 1970s showed a dramatic increase in the suicide rates and academics and health advocates at the time pointed to the introduction of highly hazardous pesticides as the culprit. Since all of the data that they have used stems from secondary and which are gathered from and up to the year 2011 one may not be able to have an understanding on impact of the civil conflict that the country faced for three decades on the suicides rates. Suicide rates in Sri Lanka are often calculated by using the Department of Police data, as it is collected nationally and many deaths by suicide occur in the community rather than in hospitals. The quality of the suicide data in Sri Lanka is unlikely to have changed over time, and there have been no research studies which have explicitly investigated whether there are cases of under-reporting in the police statistics. The most problematic issue regarding the article is that, from the outset the authors have not put any or much emphasis on why people commit suicide by using pesticides. It is in any even unsafe or unorthodox to assume that, just because of people having access to pesticides itself is a direct contributory factor for the fluctuations in suicide rates where one can never be blindfolded on other relative issues such as economical, sociological, political, cultural, ethnic and religious factors.
DISCUSSION
The article starts with a background on the suicide rates of the world, when the article was written it was nearly 800,000 deaths for a year. Most of the initial data that is produced in the article is gathered from the WHO website (“Suicide”, 2018). However, it omits to mention the fact that even today Sri Lanka is a country with one of the highest suicide rates in the world. In recent years, mainstream and social media coverage around suicide has created an impression that Sri Lanka’s suicide rate is rising rapidly. Sections of the media have begun calling Sri Lanka the ‘suicide capital’ of the world.
Others are quick to blame new technologies such as social media as the ‘cause’ for some recent youth suicides, without any research to back such claims. Sadly, public discourse is dominated by media hype, activist rhetoric and misconceptions instead of data-driven analysis. Even WHO, which sets global standards for public health analyses and responses, has erred in this regard. In September 2014, WHO’s first global report on suicide wrongly identified Sri Lanka has having the fourth highest suicide rate in the world (28.8 deaths per 100,000 according to them). That rate was modelled using data that was eight years out of date, i.e. the last national data submission made in 2006.In fact, according to the latest data released by the WHO it has a suicide rate of 34.6 suicides per 100,000 people for both the sexes. In fact, this is the highest rate of suicides in the world. One major setback that I find in this article is that it fails to define or make the reader understand as to what amounts to a suicide. Any reader who would be interested in reading an article on suicide obviously would like to know what is meant by a ‘suicide’. Shneidman defines suicide as ‘a conscious act of self-induced annihilation, best understood as a multidimensional malaise in a needful individual who defines an issue for which suicide is perceived as the best solution (Shneidman, 1993). He further elaborates on the suicide and states that, according to his perception ‘suicide has two branches. The first is that suicide is a multifaceted event and that biological, cultural, sociological, interpersonal, intrapsychic, logical, conscious and unconscious, and philosophical elements are present, in various degrees, in each suicide event. The second assertion is that, in the distillation of each suicidal event, its essential element is a psychological one; each suicidal drama occurs in the mind of a unique individual. Suicide is purposive. Its purpose is to response or redress certain psychological needs (Shneidman, 1993).
Evans and Farberow observe that ‘suicide usually took two forms: social or individual. Social suicide was generally the self-destruction of an individual demanded by a society as a price for being a member of that society. For example, sacrificing one’s life for an other is a practice found in some Eskimo tribes in which the old and sick were expected to sacrifice themselves to help ensure the survival of their group. In some primitive cultures, suicide was also a way of expressing anger and revenge in a rigidly prescribed way; for example, when a Trobriander was accused of violating atribal taboo he could climb to the top of a palm tree, name his accuser, and then jump head first from the tree. Individual suicide, on the other hand, usually occurred as a way of preserving honor, expiation of cowardice, termination of pain, preservation of chastity, escaping from personal disgrace by falling into the hands of anene my, or intense despair from separation or loss of loved ones (Evans & Far berow, 2003).
In the articleit above kind of information is not provided for the reader. One can or may argue that, such information is not required for an article such as this, but in my opinion, such a kind of introduction to suicide itself could be worthwhile to put in at the beginning of the article to arouse the interest of a reader. According to psychologists, social and mental issues contribute to persons committing suicide. Hence, they say that what is most essential is to alter people’s attitudes. The authors make an interesting observation relating to suicides in Sri Lanka, where they remark that the highest number of suicide rates were recorded in the country while it was going through a civil but however, they assume that this was not due to the civil conflict itself but was more related with the availability of pesticides in the country. This is a startling assumption to make as the authors do not look for any co-relationship with civil conflict and the suicides that were committed by individuals because of that by using pesticides to end their lives. Coming to an assumption like above lacks a broader perspective of the scenario. As it was observed by Shneidman, people use suicide as a last resort when they find no other alternative, people affected by war or a civil conflict do and indeed face many problems related to, loss of love ones, family members, companionship, loss of economic resources and means, loss of social status and livelihood and this is not exhaustive. When people lose these, they may conclude that suicide is the only option, and the means which they have used to commit suicide, whether by hanging, jumping in to a river, sea or a well, or to take highly toxicities pesticides is the means that they used to reach an end. Just because people have used a means to reach and end, we cannot conclude that the end was reached only because of the availability of the means, there are many things that attribute to an end which in this instant is about committing suicide.
The authors go on a main hypothesis, that is, if ease of access to pesticides was the main driver for the high suicide rate, the rise and fall in suicide rates would be greatest in agricultural (rural/low population density) areas because of the high levels of pesticide use (ease of access) in these locations (Knipe, Padmanathan, Muthuwatta, Metcalfe & Gunnell, 2017). However, they do not consider any of the phyco-socio issues that would be related to suicide, the coping mechanisms of the individuals in particular is not considered in their article. Empirical data relating to reasons for suicides instead of modes used for committing suicides must have been considered in the article for a better understanding of a Sri Lankan narrative on the problem. Suicide is a serious issue all over the world. Suicide is responsible for the second main reason for all the preventable deaths in the world. The world health organization observes that the link between suicide and mental disorders (in particular, depression and alcohol use disorders) is well established in high-income countries, many suicides happen impulsively in moments of crisis with a breakdown in the ability to deal with life stresses, such as financial problems, relationship break-up or chronic pain and illness. In addition, experiencing conflict, disaster, violence, abuse, or loss and a sense of isolation are strongly associated with suicidal behaviour. Suicide rates are also high amongst vulnerable groups who experience discrimination, such as refugees and migrants; indigenous peoples; lesbian, gay, bisexual, transgender, intersex (LGBTI) persons; and prisoners. By far the strongest risk factor for suicide is a previous suicide attempt. The emphasis on the reasons for committing suicides as investigated by the WHO highlights the fact that in studying suicide, it is far more important to study the reasons why people commit suicides instead of looking at the means employed by people to committing it.
In the discussion part of the article authors observe that ‘The strongest correlation between suicide rates and population density occurred in the 1980sprior to pesticide bans, at a time when access to the mosttoxic pesticides was at its highest’. Analyzing the causes of suicide can be complex. Although it would be easy to draw a direct correlation between economic status and quality of life, this is not always the case, as is visible with the countries such as South Korea and Belgium where their respective suicides rates are 24.1 and 16.1. In some countries such as Japan which has a suicide rate of 15.4, where a cultural attitude that can be described as “suicide tolerance” has been blamed. This is said to stem from a culture where the perception of others is considered more important than self-worth. Government programs have been implemented in various countries in an attempt to counter high suicide rates. These attempts usually focus on investigating the root causes of suicide in order to strategically attempt to combat it.
Prevention policies can include public awareness campaigns and an increase in funding for programs that cater to mental health. Some countries also set out to reduce social isolation among its citizens. However, this article does not touch upon any of the programmes that the governmental organizations or non-governmental organizations have implemented with regards to either preventing or minimizing suicides. Therefore, it can be argued that the reasons for a decline in the suicide rates cannot be attributed purely or mainly to the restriction or on the prohibition on the use of pesticides. It would be very irrational to make such an assumption. The article finds another somewhat interesting and a contradictory detail. Authors find that ‘district-level unemployment data were negatively correlated with suicide rates in 1971–2 and 1980–1.’. This is to say that there is no direct link between unemployment and suicide rates. This can be a truthful finding. However, it has to be also seen whether these people were though unemployed had sufficient means to sustain their selves. Sometimes unemployment would result in a decline of suicides compared to employment. When a person is employed it means that he is engaged in a money making activity and he will most times be in a room full of tension where he/she would be constantly feeling the pressures of the job and hence it can be a cause for a suicide.
Determining what causes a specific health outcome is very difficult because it is rare to be able to identify a single factor. This is particularly so for suicide. Usually there is no single cause, but a cumulation of factors which increases an individual’s vulnerability to suicide. There are, however, some clearly recognised factors that increase an individual’s risk of suicide — for example debt, job loss, a relationship breakdown, bullying, and alcohol misuse. These factors may interact with pre-existing vulnerabilities (such as mental health issues) to increase the risk of suicide. Therefore, it can be shown that it is not a good thing to just point out to a single instance such as the ease of access to pesticides as a significant contributor for the high number of suicides. Depression and disorders caused by the use of alcohol are two main factors that encourage suicides. Most young people commit suicide due to difficulty of tolerating distress associated with an interpersonal conflict. Many attempt to commit suicide due to failure in exams, failed love affairs, failure to achieve their expectations etc. One of the main reasons that people are driven to commit suicide, especially among the youth is broken love affairs. Recently, in fact a Peradeniya University Science Faculty student had thrown himself before the Badulla bound train and committed suicide.
Then just last week, a popular actor had committed suicide by hanging himself in his room where he was boarded over a love affair. Hence one cannot say that it is just the uneducated that tend to commit suicide. Even this actor was an IT graduate. Since 1996 when the special Presidential Task Force set up the National Policy on suicide prevention, it is recognized that mental illness, alcohol and drug use, poor coping skills, are all contributory factors that lead people towards suicide in Sri Lanka. Services are therefore targeted towards helping people who fall into these categories. The fact that suicide is invariably the outcome of a combination of factors – environmental, psychological, sociological and biological is now accepted. Suicide is not something that can be condoned nor accepted. No matter what the issue is that is worrying a person, suicide is never the answer. However, some reach a stage of desperation that they feel that they are unable to cope with the problem and think that suicide would put a stop to their pain and suffering, forgetting the burden and pain it causes those who love them such as their families. Evidence is mounting that genetic factors may be included in the many determinants of suicide. Clinical studies of psychiatric patients have suggested that risk of suicidal behavioris increased by the presence of family history of suicide. The genetic susceptibility to suicide, however, tends to affect individuals only in association with stress or psychiatric illness. Around 35-58 % of suicides are attributed to genetic factors. Those affected by the war too are more prone to suicide, having gone through many harrowing experiences. Alcoholism is also a huge contributory factor in suicide. Suicide is an escalating public health problem, and alcohol use has consistently been implicated in the precipitation of suicidal behavior. Alcohol abuse may lead to suicide through disinhibition, impulsiveness and impaired judgment, but it may also be used as a means to ease the distress associated with committing an act of suicide.
According to the Penal Code paragraph 302 suicide is an offence but since it has no direct bearing on society it is not implemented properly. Yet it is something that sets a bad example and as we have seen in the recent past, young children too are attempting suicide even for trivial reasons. They get the notion perhaps that suicide is the end to their problems or pain. Hence those prone to suicide should be assessed and treated in time, so that it can be prevented. In fact, those prone to commit suicide either talk about it way before they attempt it or show signs of distress. Therefore, it is important to access these situations at the right time and provide the necessary treatment to those who require it. Currently in families both mother and father are occupied with earning and providing for the family that often children are either left alone or with servants. Hence, these children are withdrawn and distant from the family. This makes it hard to either parent to notice changes in a child’s behavior until eventually the child commits suicide which then is too late. The family fabric in this country has somewhat been damaged in the pursuit of materialistic requirements. Sri Lanka was once known as a majestic nation where only the brave sacrificed their lives for the country. However, now many are opting to commit suicide unable to face life and its challenges. Family is where this problem can first be detected. Hence, it is important for families to forge that closeness between children and parents, so that children can come to their parents when they are disturbed or distressed and parents too need to be available for their children in such instances. Suicide is certainly not an option and this should be inculcated in the minds of our children. They must be made to understand that there is always a solution to any problem and it can be dealt with and suicide is not the solution. Education should not just be limited to books and mental strength and the right attitudes should be inculcated in our younger generation to make them resilient mentally.
Sri Lanka is far ahead of her South Asian neighbors in the accomplishment of human development goals. Life expectancy at birth is currently 72 yrs. and is close to the estimated lifespan in the developed countries. High literacy rates, low mortality rates and the steadily declining population growth, reflect the country’s progress in the sphere of social development. All these human development indicators are a tribute to Sri Lanka’s social service network, which was established in the latter part of the 1940 decade, ensuring sound educational policies, an extensive health care programme and an effective medical system for all sectors of the nation. The question then arises as to why such a country with a great track record relating to other social indicators struggles with the rate of suicides. Sri Lanka ranks first among South-East Asian countries with respect to commitment of suicide. Poverty, destructive pastimes and inability to cope up with stressful situations, are the main causes which tend to the sudden ending of human life in this tragic manner. The following depicts the Suicide rate by age group
DEPICTS THE SUICIDE RATE BY AGE GROUP
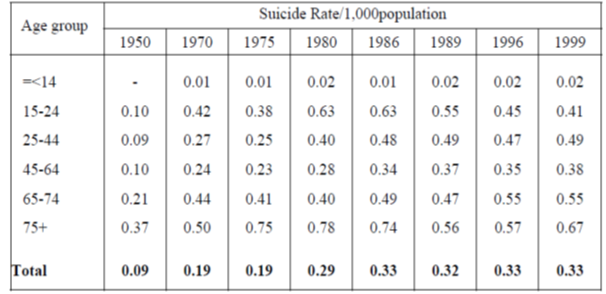
The above data clearly indicates that there is a vulnerable age group in the ranges as the suicide rate is at its highest at the age of 75 and above. While the second highest rate is associated with ages 64-75 it is interesting to note that between the ages of 45-64 the rate of suicide is significantly lower. So if we were to think that the access to pesticides itself was the reason for this number of suicides it will not provide a clear picture as for the variation in the rate of suicides between the ages. The reason for this is that, there is no barrier for people living in these ages to accessing pesticides. The reason for these variations could lie in the fact of different coping strategies that people will use in facing problems. While old age itself may be a reason for committing suicides due to lack of care and attention, what is remarkable is that the lowest number of suicides are recorded for the ages of 45-64. This epitomizes the fact that, when people reach this age level, their level of experience and coping mechanisms are better than at the other levels, and the problems they face would be nothing new to them.
CONCLUSION
A civil war that spanned over 25 years (1983-2009) left the country in social disintegration with an estimated 100,000 lives lost. Suicide rates were highest during the war and a significant reduction was established in post-conflict Sri Lanka. Financial hardship and loss of livelihoods was repeatedly affected families especially in the Northern provinces, numerous individuals suffered from depression and posttraumatic stress disorder (PTSD) and many more resorted to suicide.
A mental health stigma still exists in Sri Lankan society. Patients are subjected to discrimination, especially by employers, which have only proven to exacerbate the condition. Self-stigmatization has led to significant delays in seeking aid; patients were often withdrawn opting for secrecy rather than disclose any emotions. Fernando et al stated that doctors have also shown to have stigmatizing attitudes towards depression and alcohol and drug addiction patients. Sexuality plays an undeniable part in suicide. Homophobia is common amongst families, they disown and force out homosexuals, who then face a lot of discrimination by relatives and society in general, and many have opted for suicide due to the constant torment and mental stress. Engaging in homosexual acts is currently against the law and is punishable by up to 10 years in jail Even today private clinics exist with the sole aim of ‘curing’ homo sexuality. Such findings call for anti-stigma campaigns for the LGBT community and certain mental health disorders. General education for the public is vital and also efforts must be made to reduce poor attitude towards mental health disorders in medical education. Youth unemployment has always been a huge burden in Sri Lanka and is a considerable suicide factor. Education system in Sri Lanka is highly competitive and is often criticized for overly academic orientated. Efforts have been made to modernize the program by offering apprenticeships and career opportunities. Nevertheless over 20% of the youth remain unemployed. The highly competitive nature of education alongside deteriorating relations with parents and the desire to prove one’s self-worthiness has shown to be detrimental on the mental health of the youth. Therefore, psychosocial support and services focusing these matters are essential in tackling youth suicide rates.
The media is an influential role on suicide, it can be aid in the public awareness of suicide and mental health or it can promote suicide by portraying it as a means of escaping hardship and suffering. Journalists must adopt a sensitive approach when reporting on suicide cases as they have shown to be highly influential on the younger generation who are able to relate to the situation. A conflict-ridden history has meant that suicide has become a common method to escape a distressed and psychologically unbearable life. Tackling suicide in Sri Lanka necessitates a multifaceted approach. Means restriction has proven to be extremely effective; the introduction of legislation prohibiting the most toxic of pesticides greatly impacted suicide mortality. Lockable safe storage of pesticides represents another effective strategy but these distal interventions have shown to potentiate means substitution. Therefore, tackling the proximal determinants of suicidal behavior is paramount.
However the current understanding of these factors is limited, the rising cost of living and the social stresses due to education and employment have shown to be contributory to the suicide burden. Cultural ideology and stigma surrounding aspects such as mental health and sexuality have shown to hinder progress. A lack of public awareness and understanding exacerbates the issue; therefore public education campaigns are vital interventions. Current governmental mental health policies are commendable but a lack of human resources is apparent. Task shifting provides a potential alternative but the social hierarchy and attitude towards delegation of authoritative figure roles to less qualified individuals proves to be a major barrier. The task at hand is vast, as it essentially requires a social revolution, but the combined efforts of the government, the general public and NGOs would positively impact the persistent suicide problem in Sri Lanka.
The man who kills a man kills a man. The man who kills himself kills all men. As far as he is concerned, he wipes out the world.
BIBLIOGRAPHY
- Evans, G., & Farberow, N. (2003). The encyclopedia of suicide (2nd ed.). New York: Facts On File.
- Knipe, D., Padmanathan, P., Muthuwatta, L., Metcalfe, C., & Gunnell, D. (2017). Regional variation in suicide rates in Sri Lanka between 1955 and 2011: a spatial and temporal analysis. BMC Public Health, 17(1). http://dx.doi.org/10.1186/s12889-016-3961-5
- Shneidman, E. (1993). Suicide as psychache (1st ed.). Northvale (NJ): Jason Aronson
- Suicide. (2018). World Health Organization. Retrieved 19 April 2018, from http://www.who.int/mediacentre/factsheets/fs398/en/