
Diagnostic and Potential in Assisting Therapeutic Decisions of N-Terminal Pro B-Type Natriuretic Peptide Levels in Patients with Suspected Congestive Heart Failure at Parirenyatwa Group of Hospitals In Harare, Zimbabwe
- Terrence Nyamayaro
- Courage Mpandawana
- 2794-2818
- Aug 9, 2025
- Education
Diagnostic and Potential in Assisting Therapeutic Decisions of N-Terminal Pro B-Type Natriuretic Peptide Levels in Patients with Suspected Congestive Heart Failure at Parirenyatwa Group of Hospitals in Harare, Zimbabwe
Terrence Nyamayaro, Courage Mpandawana
University of Zimbabwe
DOI: https://dx.doi.org/10.47772/IJRISS.2025.907000229
Received: 27 June 2025; Accepted: 04 July 2025; Published: 09 August 2025
ABSTRACT
Background: Heart failure is a clinical syndrome caused by structural and functional defects in the myocardium resulting in impairment of ventricular filling and/ or the ejection of blood. Natriuretic peptides have emerged as important tools for diagnosis, risk stratification and therapeutic decision making for patients with heart failure. Relative changes in the amino-terminal pro B-type natriuretic peptide (NT-proBNP) levels may assist in the assessment of the risk of congestive heart failure (CHF). However, whether the levels can enable the prediction of outcomes with acute exacerbation at the time of admission remains unknown. This study seeks to determine the diagnostic and therapeutic potential of NT-proBNP in the diagnosis of CHF at Parirenyatwa Group of Hospitals. The study will also determine the correlation between NT-proBNP measurement and the gold standard method for the diagnosis of CHF.
Methods: Patients suspected to have CHF who were admitted at Parirenyatwa Group of Hospitals’ medical wards and urgent care unit who had requests for echocardiogram were enrolled into the present cross-sectional study. All patients had dyspnoea of differing severity. The mean age of the participants was 71±7 years old. Demographic data was collected using a pretested interviewer-based questionnaire. Four millilitres of blood sample were collected from each participant into sodium citrate tubes and sent to GoPath Clinical Laboratories. Plasma levels of NT-proBNP were immediately measured, and other risk factors, symptoms and clinical data were also investigated. The sensitivity, specificity, diagnostic accuracy, positive predictive value and negative predictive value of the NT-proBNP assay amongst patients suspected to have CHF was determined. The performance of the assay was also evaluated against the gold standard method.
Results: Of the 110 patients, 74 (67.3%) had CHF. The remaining 36 (32.7%) presented with dyspnoea of non-cardiac origin. Plasma NT-proBNP levels were higher in patients with CHF (492.5, IQR= 300.0 – 709.0 vs 49.5, IQR = 34.5 – 69.5; P<0.001), and increased as functional status deteriorated (P=0.0001). The area under the receiver operating characteristic curve was 0.9448 for the optimum cut-off value of 100 pg/ml. The sensitivity for this cut-off value for diagnosing CHF was 97.3%, the specificity was 91.7%, the positive predictive value (PPV) was 96.0%, and the negative predictive value (NPV) was 94.3%.
Conclusion: Findings from the current study demonstrates the importance of plasma NT-proBNP in the diagnosis and exclusion of CHF in dyspnoeic patients. Plasma NT-proBNP has proved to be an important biomarker which can be used to assess diagnosis and severity of CHF as well as to potentially guide therapy in CHF patients. It is a simple, inexpensive, useful and highly effective diagnostic test for CHF. Although echocardiography remains the gold standard method regarding the provision of detailed information on cardiac performance and structure, imaging data alone is not sufficient enough to identify patients with adverse CHF outcomes. An integrated approach which can combine laboratory assays with imaging and clinical presentation will greatly improve the diagnosis of CHF.
Keywords: Diagnostic potential; N-terminal pro B-type natriuretic peptide; Congestive heart failure, Parirenyatwa Group of Hospitals.
INTRODUCTION
Introduction
Pro B-type natriuretic peptide (Pro-BNP) is a 108 amino acid polypeptide which is secreted by myocytes as secretory granules in both the right and left ventricles of the heart, and to a lesser extent, in the atria (1, 2). It is secreted into ventricles in response to volume expansion and pressure overload, and it breaks down into its two cleaved forms; N-Terminal pro B-type natriuretic peptide (NT-proBNP), which is a 76-peptide biologically inert N-terminal fragment, and B-type natriuretic peptide (BNP), which is a 32-peptide biologically active hormone (1). NT-proBNP has a central role in the regulation of blood pressure, blood volume and sodium balance (2). Its levels increase with age, ventricular hypertrophy and in acute syndromes, Heart failure, and atrial fibrillation (2). BNP also has an important role in regulating blood circulation as it acts on blood vessels, causing them to dilate or widen.
Multiple studies have previously investigated on the utility of NT-proBNP in the diagnosis and prognosis of CHF, and/ or its association with the occurrence of CHF (3, 4, 5, 6).
In the year 2000, the United States Food and Drug Administration (US-FDA) approved BNP as an adjunct to diagnose heart failure. In the same year that Biosite Inc (now Alere) introduced the test as a point of care assay for use in emergency departments (7). Since then, BNP and NT-proBNP have been used for the diagnosis of heart failure, in triage and as a guide to treatment and discharge of patients with heart failure (7).
The past years have seen an increase in the use of natriuretic peptides in patients with coronary heart disease (CAD), valvular heart disease, severe sepsis, septic shock, renal failure, liver cirrhosis and several other pulmonary conditions (7). According to studies by Costello-Boerrigter et al in 2005 (8) and Jarolim in 2006 (9), the levels of BNP and NT-proBNP at the time of discharge from hospital were important in the prediction of long-term outcomes among patients with CHF. However, both studies (8, 9), could not explain the significance of the levels of BNP and NT-proBNP at the time of admission (10).
Both NT-proBNP and BNP are now known to have clinical significance as diagnostic and prognostic markers in the management of Heart Failure (1). In the diagnosis of Heart Failure in patients presenting with dyspnoea, BNP levels less than 100 pg/ml have a 90% negative predictive value (NPV) and values greater than 500 pg/ml have an 81% positive predictive value (PPV) (3). Plasma BNP levels can be used as a strong predictor of the risk to death and cardiovascular events in patients previously diagnosed with heart failure or cardiac dysfunction (1). Patients with renal failure, pulmonary embolism, pulmonary hypertension and chronic hypoxia are associated with elevated BNP levels, whilst obese and overweight individuals have relatively lower BNP levels (1). BNP and NT-proBNP have shown no clinically significant difference in terms of the diagnostic and prognostic values (11). However, NT-proBNP has a longer half-life (72 hours) as compared to the 4 hours for BNP, and its levels are less affected by obesity (11).
Background to the study
The pathogenesis of heart failure is caused by structural and functional defects in the myocardium resulting in impairment of ventricular filling and/ or the ejection of blood (1, 12, 13, 14). It is most commonly caused by reduced ventricular myocardial function. However, the dysfunction of the pericardium, myocardium, heart valves or great vessels alone or in combination has also been associated with heart failure (12, 13, 14).
Patients usually present with dyspnoea, shortness of breath, fatigue, reduced exercise tolerance, fluid retention, arrythmias, chest tightness, palpitations, unreasonable breathlessness, neck vein dislocation (NVD) and orthopnoea (12, 13, 14). CHF is caused by structural abnormalities of the heart, functional abnormalities, and other triggering factors (12).
An incorrect diagnosis for acutely ill patients presenting to the emergency department with dyspnoea will place the patient at risk for both morbidity and mortality.
About 800 000 people in the United Kingdom currently have heart failure, with more than 250 000 new cases being detected every year (15). Incidence rates increase with age and is highest in adults aged 75 years and above (15). The aging population and improved survival of people with ischaemic heart disease (IHD) are factors likely leading to continuing increase in the prevalence of heart failure (15). In sub-Saharan Africa (SSA), CHF remains a major health challenge, often presenting as an emergency, and it is the most predominant primary diagnosis for patients admitted with cardiovascular disease requiring significant hospitalisation (16, 17, 18, 19, 20, 21).
In the last decade, CHF has featured in several multinational studies in three countries in North Africa (Tunisia, Algeria and Egypt) and nine countries in SSA (Senegal, Nigeria, South Africa, Mozambique, Uganda, Kenya, Ethiopia, Cameroon and Sudan) (22, 23, 24, 25, 26, 27). HF epidemiology from all medical admissions varied widely, from 9.4% to 42.5% in Nigeria (28, 29) and 12.2% in Tanzania (19). One study in Tanzania reported that HF was responsible for 1.9% of all cases presenting to the emergency department (30). Furthermore, meta-analysis indicated that between 25.6% and 30.0% of admissions to cardiac units were attributable to HF in SSA (16, 31). Other studies in countries in SSA that reported HF epidemiology from admissions to cardiac units, included Sudan 12.0% (32), Togo 28.6% (33) and Cameroon 30.0% (34). Accordingly, CHF has emerged as a dominant form of cardiovascular disease in SSA (35).
Over the past two decades biomarkers have emerged as important tools for the diagnosis, risk stratification and therapeutic decision making in cardiovascular diseases (4, 5, 6, 7). They do not only provide valuable information about the pathophysiology of the disease, but they also shed light on the severity of ongoing disease. Guidelines from the National Institute for Health and Clinical Excellence, and the European Society for Cardiology (ESC) on the initial diagnosis of CHF and referral for echocardiography recommended the use of BNP tests in combination with clinical assessment (15, 36, 37).
A previous review by Simons et al. (38) on the criteria and cut off values for the diagnosis, prognosis and treatment guidance found out that single measurements of natriuretic peptides, BNP ≤ 100pg/ml or NT-proBNP 300 pg/ml, rules out heart failure, while BNP ≥ 100 pg/ml or NT-proBNP ≥ 300 pg/ml have been proposed to have a relatively lower level of evidence in clinical settings (38). Both BNP and NT-proBNP levels can therefore be used to aid in decisions regarding admission, discharge and risk stratification for heart failure patients. Patients with BNP levels less than 200 pg/ml at admission have been associated with a 2 % mortality rate as opposed to a 9 % mortality rate associated with patients admitted with BNP levels greater than 200 pg/ml (39). NT-proBNP levels of 5000 pg/ml or higher at admission have been shown to be associated with an in-hospital mortality rate of 22.5 % and longer length of stay for surviving patients (40).
LITERATURE REVIEW
Natriuretic peptides have emerged as important tools for diagnosis, risk stratification and therapeutic decision making for patients admitted at emergency cardiac units (4, 7). Biomarkers such as BNP and pro-BNP have become very important in the evaluation of the risk of congestive heart failure (CHF) (41, 42, 43, 44, 45, 46, 47). An understanding of the level of BNP and NT-proBNP may provide an early diagnosis and guide for CHF therapy (41, 42, 46).
The main stimulus for increased BNP and NT-proBNP synthesis and secretion is myocardial wall stress (4, 12, 14). Both molecules can be detected in blood (4). Upon release into circulation proBNP is cleaved into equal proportions of BNP and NT-proBNP (4, 12, 14). BNP is cleared from plasma by binding to the natriuretic receptor peptide type C (NPR-C) and through proteolysis by neutral endopeptidases, whereas NT-proBNP is mainly cleared by renal excretion (4). This, coupled with a longer half-life of 120 minutes for NT-proBNP compared to the 20 minutes for BNP results in NT-proBNP values being approximately six times higher than BNP in blood (Figs 1 and 2) (4).
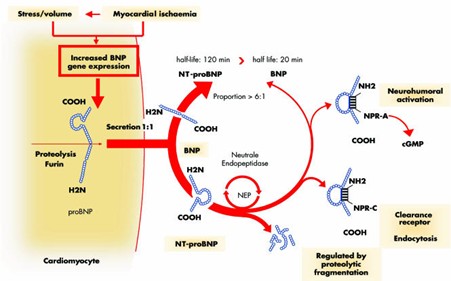
Figure 1. BNP and NT-proBNP synthesis, release and receptor interaction (4). Reproduced with permission from E Spannuth.
Figure 1. above shows a schematic illustration of B-type natriuretic peptide (BNP) and NT-proBNP synthesis, release and receptor interaction. As shown on the diagram, BNP is produced as a prohormone in the cardiomyocytes and upon release into circulation, pro-BNP is cleaved into BNP and NT-proBNP in equimolar proportions. Interaction of BNP with the natriuretic peptide receptor type A (NPR-A) mediates the biological effects via intracellular cyclic Guanosine Monophosphate (cGMP) increase (4). Binding of BNP to NPR-A leads to an increase in intracellular cyclic GMP (cGMP), which mediates the biological effects of BNP. As shown in Figure 1. BNP can also bind to the clearance receptor, natriuretic peptide receptor C (NPR-C), and to lesser extent to NPR-B (guanylyl cyclase B). BNP, through NPR-A activation, leads to vasodilation, increased excretion of sodium and water by the kidneys (natriuresis and diuresis), and suppression of the renin-angiotensin-aldosterone system (RAAS)

Figure 2. Physiological effects of B-type natriuretic peptide (BNP) (4).
As shown in figure 2, volume or pressure overload leads to ventricular wall stress and BNP release. The systemic biological effects of BNP are peripheral vasodilation, increase in natriuresis, and inhibition of the sympathetic nervous system (SNS) and the renin-angiotensin-aldosterone system (RAAS) (4). These effects will help reduce blood pressure, blood volume, and overall workload on the heart. BNP’s actions are beneficial especially in conditions like heart failure, where they help counteract the effects of fluid retention and increased sympathetic activity.
Several studies have investigated the association of NT-proBNP with an occurrence of CHF (1-7). Studies by Dai et al in 2017 (41), Richards & Troughton in 2004 (48), Hayek & Nemer in 2011 (49) and Valle & Aspromonte in 2010 (50) have all demonstrated NT-proBNP as a strong predictor of CHF, and they have also proved that it provides greater stability and more information as compared to BNP, owing to its longer half-life.
The NT-proBNP investigation of dyspnoea in the emergency department (PRIDE study) by Januzzi et al in 2005 (51) and the International Collaborative of NT-proBNP study (ICON study) by Januzzi et al in 2006 (52) have both shown the diagnostic value of NT-proBNP in CHF, and this is presented in table 1 below.
Table 1. Diagnostic performance of NT-proBNP in CHF (41).
| Studies | Number | Diagnosis of Heart failure | Analysed | Cut-off (pg/ml) | Sensitivity | Specificity | PPV | NPV |
| Januzzi (PRIDE) | 599 | Clinical | NT-proBNP | 300 | 99 | 68 | 62 | 99 |
| Januzzi (ICON) | 1256 | Clinical | NT-proBNP | 300 | 99 | 60 | 77 | 98 |
Key: PPV: Positive predictive value (in percentage), NPV: Negative predictive value (in percentage), CHF: Congestive heart failure, NT-proBNP: N-terminal pro-brain natriuretic peptide, PRIDE: NT-proBNP investigation of Dyspnoea in the emergency department, ICON: International Collaborative of NT-proBNP study.
As shown in table 1, NT-proBNP had a sensitivity of 99% in both studies with a cut-off value of 300 pg/ml. Its specificity was 68% in the PRIDE study and 60% in the ICON study, and the PPV and NPV were also as shown on the table.
More recent studies in by Onyemelukwe et al. (53) and Sani et al. (54) have demonstrated the potential role of NT-proBNP in the diagnosis and prognosis of CHF in SSA. The 2022 American College of Cardiology, American Heart Association and the Heart Failure Society of America (ACC/ AHA/ HFSA) and the 2021 European Society of Cardiology (ESC) HF guidelines recommended the use of natriuretic peptides to support the diagnosis of HF (55, 56, 57). Further studies are still needed to fully establish the role of NT-proBNP in CHF diagnosis, and this study aims to determine the diagnostic potential of NT-proBNP in the diagnosis of CHF amongst the Zimbabwean population.
Statement of the Problem
If treated appropriately in the early stages of the disease, heart failure may be reversible, thus early diagnosis is very important (15). Despite the advancement in medicine and diagnostic procedures, the management of heart failure, which usually presents as a disease syndrome, is still a challenge to healthcare providers (1). This can be reflected by the relatively higher rate of readmissions and increased mortality and morbidity rates associated with heart failure. Echocardiography is currently considered as the gold standard method for diagnosing left ventricular dysfunction but, however, it is very costly and it has limited availability in urgent-care settings. It may also not always reflect an accurate condition due to its non-specific nature (15, 58, 59). Over the past years, Doctors in Zimbabwe have over-relied on echocardiography as the main diagnostic test for CHF which has resulted in delays in disease diagnosis, and sometimes unnecessary loss of life as relatives fail to pay the huge amounts required for the test or due to the common issue of machine breakdowns which have become very common at PGH radiology. Since early diagnosis and timely initiation of guideline-directed medical therapy are paramount to mitigating these poor outcomes, there is need to address these challenges. Finding a rapid and simple cost-effective blood test that would aid in the diagnosis and management of patients with CHF would have a favourable impact on the staggering costs associated with the disease and delays in disease diagnosis (60, 61).
Research question
Can NT-proBNP be used as a diagnostic biomarker in patients with suspected CHF?
Hypothesis
NT-proBNP can be used as a diagnostic biomarker for CHF.
Study Aim
To determine the potential of NT-proBNP in the diagnosis and in assisting therapeutic decisions in patients with suspected CHF.
Study Objectives
- To determine the levels of NT-proBNP in patients suspected to have CHF at Parirenyatwa Group of Hospitals.
- To determine the correlation between NT-proBNP and the gold standard method for the diagnosis of CHF.
- To evaluate the sensitivity and specificity of NT-proBNP test against the gold standard method.
Justification of the study
NT-proBNP and BNP have clinical significance as both diagnostic and prognostic markers in the management of heart failure (1). Previous data has suggested that serial point-of-care testing of NT-proBNP can immensely help patients presenting to emergency care clinics with dyspnoea (60). It might serve as a screening test for patients referred for echocardiography and might also be an effective way of improving in-hospital management of patients admitted with CHF (60). NT-proBNP may offer an alternative and cheaper option to echocardiography as it can be readily available in emergency care settings. The test will also benefit patients at Parirenyatwa (PGH) as the hospital is currently struggling with echocardiography machines which are constantly breaking down.
Currently, there is no clear consensus about the appropriate BNP threshold for diagnosing CHF in Zimbabwe and no current reliable studies have been conducted in the Zimbabwean context, to determine the utility of NT-proBNP in the diagnosis of CHF in the Zimbabwean population. Thus, useful information will be obtained from the results of this study project. Finally, if favourable results are obtained from the study, it will make it easy for policy makers to endorse the use of the test as a screening tool for CHF. The introduction of the test as the base-line screening test for CHF will in turn benefit patients and the medical practice at large by providing quick bed-site results which will in turn assist with early disease diagnosis.
METHODOLOGY
Study Design
Since this topic has not been previously studied in depth in the Zimbabwean context, an exploratory cross-sectional study was conducted at Parirenyatwa Group of Hospitals. This type of study design was used in this study because it was less costly and could be done in the short space of time which was available, yet it can measure multiple variables at the time of the data snapshot producing findings which can generate a hypothesis which can be tested in further research studies.
Study Setting
The study was conducted at Parirenyatwa Group of Hospitals (PGH) medical wards and urgent care unit between September and October 2022. PGH is the major referral centre in Harare, Zimbabwe, which is a developing country in Southern Africa with a population of about 13 million people according to the 2013 census report (ZIMSTAT., 2013). It has a gross national index per capita of US$860 with 72.3% of the population living below the national poverty line (The World Bank., 2015).
PGH is the major referral centre in Harare, Zimbabwe, and it is the largest medical centre in Zimbabwe thus it offers a population diversity. It has a daily occupancy of between 950 to 1000 patients per day. The facility has general medical and surgical sections, Mbuya Nehanda, the maternity section, Sekuru Kaguvi, which specialises in eye treatment; and an annex for psychiatric patients and several specialist paediatric wards. It has an excess of 5000beds and 12 theatres in the main hospital complex. There is also the opportunistic clinic section where PLHIV come for routine HIV care. PGH also has a 24-hour operating accident and emergency department. All these departments are supported by auxiliary services such as the laboratory, pharmacy and physiotherapy.
Sample collection was carried out at the medical wards and urgent unit care with N-Terminal pro B-type natriuretic peptide concentrations measured at GoPath Clinical Laboratories’ main branch in Harare, Zimbabwe. GoPath Clinical Laboratories is one of the main private laboratories in Zimbabwe, and it offers pathological testing in all departments which include Microbiology, Serology, Haematology, Biochemistry, Immunochemistry, Histology and Cytology.
Both PGH and GoPath Clinical Laboratories are located in an easily accessible area which were within the researcher’s reach.
Figure 3. Study setting, PGH
Study Population
Patients presenting with clinical signs and symptoms of heart failure or CHF and who had been referred for echocardiography at PGH were recruited to participate in the study.
Inclusion and Exclusion Criteria
Inclusion Criteria
Consenting patients meeting the clinical assessment case definition of heart failure, and aged 18 years or more, and who have been referred for echocardiography were included in the study.
Exclusion Criteria
Patients not meeting the clinical assessment case definition of heart failure, non-consenting patients and those aged less than 18 years were excluded from the study. Patients with no requests for echocardiography, patients with a history of renal failure, pulmonary embolism, pulmonary hypertension, chronic hypoxia and those who were previously diagnosed with heart failure or other problems associated with dyspnoea were also excluded from the study.
Sample Size Calculation
A minimum sample size of 95 participants was sufficient for the study and this was obtained by using the Dobson formular (62);
![]()
Where;
n is the minimum sample size
P is the prevalence of the condition/ health state based on previous literature, (P = 0.44)
d is the precision of the estimate (d = 0.1), and,
Zα is the Z-value from the probability tables, that is alpha = 5% (Z = 1.96)
Using assumptions from a study by Taylor, et al. (15), where the prevalence of CHF in primary care varied from 19% to 44%, a 10% margin of error, a confidence interval (CI) of 95% and a non-response rate of 10%, a minimum sample size of 95 patients was calculated. However, to cater for possible drop-outs due to exclusion criteria and to possibly increase the power of the study, a sample size of 110 patients was used for the study.
Sampling Procedure
A systematic random sampling technique was used, where consenting patients meeting the clinical assessment case definition of heart failure were enrolled into the study. Every second patient/ bed at PGH medical wards and urgent care unit was selected for the study, and in the event the participant chose not to participate, the next patient/ bed in line was selected until one hundred and ten patients were recruited into the study. Four millilitres of blood samples were drawn into pre-chilled sodium citrate tubes and immediately sent to the laboratory for processing.
Data Collection
Data collection tools
Interviewer-administered questionnaires were used as data collection tools and these were pretested using the respondent-driven pretesting method prior to actual sample collection. The questionnaire was divided into two sections. Section A consisted of the sociodemographic characteristics of the patient and this included the name, date of birth, age, gender, ethnicity, religion and identification number. Section B consisted of questions regarding the signs and symptoms of CHF; any risk factors and any history of renal failure, pulmonary embolism, pulmonary hypertension or chronic hypoxia. The study participants were also asked if they had ever had an abnormal ECG or echocardiogram before. Height and weight data were used to calculate body mass index (BMI). Prior to section A, there was a brief explanation of the study topic and instructions. The questionnaire was available in both English and Shona languages and some of the patient’s history was provided by the Doctor from the patient’s ward notes.
Pretesting of the data collection tool
The interviewer administered questionnaire was pretested prior to data collection using the respondent-driven process. This was to determine the potential effectiveness of the questionnaire and also to check if the respondents were able to understand the questions. Eleven random patients suspected to have CHF were selected from PGH medical wards and asked to complete the questionnaire, taking note of the time they took to respond and the way they responded. Eleven respondents were selected as they were deemed enough to warrant significant results since they represented 10% of the projected sample size for the study.
Data Collection Procedure
Potential participants were first introduced to the study and its requirements before being asked questions based on the pretested interviewer-administered questionnaire. This allowed a proper screening of the respondents so that only those presenting with clinical signs and symptoms of heart failure were enrolled into the study. If confirmed suitable to participate, participants were asked to complete an informed consent which was followed by sample collection. The data collection procedure only lasted 10 to 15 minutes per respondent. The collected blood sample was placed in a zip lock biohazard specimen bag, each sample being placed in a different labelled biohazard specimen bag, and these were packed in a biosafety transport box and send to the laboratory for processing. No special treatment of the specimen was required at this stage since the samples were transported as whole blood. A bed-site/ desk review of medical records was done for additional data extraction, and this included data on the height, weight, blood pressure and diabetes status of the participating patients. BMI was calculated using height and weight data obtained from the patients’ medical records. Cardiac structure and function were determined following a standard echocardiography. The diagnosis of CHF was finally pronounced by a specialist physician, who was blinded to the NT-proBNP concentrations. A New York Heart Association (NYHA) functional classification was first assigned to the patients by the specialist physician, and this is a heart failure grading scale which is used to assess the severity of possible heart failure patients based on limitations during physical activity.
Covid-19 prevention protocols such as social distancing, wearing of face masks and use of alcohol-based hand sanitizer were observed before, during and after the data and sample collection procedures. During sample processing, the researcher observed the use of personal protective equipment such as laboratory coats, nitrile gloves, face masks and goggles. Wastinnova Biohazard Waste Disposal Services private limited company was responsible for the disposal of the samples after sample processing.
Laboratory Methods
Plasma sample was obtained by centrifuging the sodium citrate tubes at 3000 rpm for 5 minutes in a centrifuge (Yingtai Instrument, China). This was done within 30 minutes after sample collection, and processing was done within an hour after sample collection.
Plasma NT-proBNP
Plasma NT-proBNP concentration was measured using the Getein 1100 immunofluorescence quantitative analyser (Biotech, Inc) according to the manufacturer’s instructions. This test uses an anti-human NT-proBNP monoclonal antibody conjugated with fluorescence latex and an anti-human NT-proBNP polyclonal antibody coated on the test line. After application of the sample to the test strip, the fluorescence latex-labelled anti-human NT-proBNP monoclonal antibody binds with the NT-proBNP in the sample to form a marked antigen-antibody complex. This complex moves to the test card detection zone by capillary action and it is captured on the test line by the anti-human NT-proBNP polyclonal antibody. The fluorescence intensity of the test line will increase in proportion to the amount of NT-proBNP in the sample. The Getein 1100 immunofluorescence quantitative analyser will measure the concentration of NT-proBNP in the sample and display the concentration on the screen in pg/ml.
Performance characteristics of the Getein 1100 immunofluorescence quantitative analyser
- Measuring range: 50 – 35000 pg/ml
- Lower detection limit: ≤50 pg/ml
- Within-run precision: ≤10%
- Between-run precision: ≤15%
These performance characteristics were provided by the kit manufacturer and verified before the initiation of the research study. Quality control materials were also included in every run.
NT-proBNP values less than 50 pg/ml were rerun using the Maglumi 800 Immunoassay analyser (Snibe Co. Ltd) to obtain the actual quantitative values. The analyser uses the sandwich immunoluminometric assay, where an anti-NT-proBNP monoclonal antibody is used to label ABEI, and another monoclonal antibody is used to label magnetic microbeads. The sample, calibrator or control, ABEI label and magnetic beads coated with anti-NT-proBNP are then mixed thoroughly and then incubated at 37ºC to form a sandwich, after sediment in a magnetic field. Starter reagents are then added and a flash chemiluminescent reaction is initiated. The light signal is measured by a photomultiplier as relative light units within 3 seconds and this is proportional to the concentration of NT-proBNP in the sample. Prior to use of the Maglumi 800 immunoassay analyser, 5 random samples were selected and run to check for the consistence of the results with those processed on the Getein 1100 quantitative immunofluorescence analyser.
Performance characteristics of the Maglumi 800 immunoassay analyser
- Measuring range: 0 – 2500 pg/ml
- Lower detection limit: 0 pg/ml
- Within-run precision: ≤10%
- Between-run precision: ≤15%
These performance characteristics were provided by the kit manufacturer and verified before the initiation of the research study. Quality control materials were also included in every run.
Preferred Cut-off values
A participant was considered to be free from heart failure if NT-proBNP was less than 100 pg/ml, heart failure if NT-proBNP was at least 100 pg/ml and moderate heart failure if NT-proBNP was greater than 600 pg/ml as shown below:
- <100pg/ml: No heart failure
- 100-300pg/ml: indicates mild heart failure
- >300pg/ml: moderate heart failure
- >600pg/ml: severe heart failure
These values were obtained from the values recommended by the kit manufacturer.
Study Parameters and Outcomes
The utility of NT-proBNP in assessing patients with possible heart failure was investigated. The effect of various determinants such as age and gender on the diagnostic performance of NT-proBNP was also investigated. The following parameters and/ or outcomes were assessed as part of the evaluation for the diagnostic performance:
CHF
CHF was the primary outcome variable and it was defined as a complex clinical syndrome characterized by exercise intolerance, due to the heart failing to pump blood as it should be, and/ or signs of congestion in the presence of a cardiac condition (29, 30). A New York Heart Association (NYHA) functional classification was first assigned to the patients by the specialist physician, and this is a heart failure grading scale which is used to assess the severity of possible heart failure patients based on limitations during physical activity. It placed patients in one of four categories based on how much they were limited during physical activity. Table 2 below shows the NYHA functional classification. An echocardiography was used as the gold standard method for diagnosis of CHF. NT-proBNP was the other parameter and an NT-proBNP level of 100 pg/ml was considered the cut-off value for CHF.
Table 2. NYHA functional classification (63).
| CLASS | PATIENT SYMPTOMS |
| I | No limitation of ordinary physical activity. Ordinary physical activity does not cause undue fatigue, palpitations or dyspnoea. |
| II | Slight limitation of ordinary physical activity. Patient comfortable at rest. Ordinary physical activity results in fatigue, palpitations, dyspnoea or shortness of breath. |
| III | Marked limitation in activity. Patient comfortable at rest. Less than ordinary activity causes fatigue, palpitations or dyspnoea. |
| IV | Severe limitations in activity. Patient unable to carry on any physical activity without discomfort. Symptoms of heart failure occur even at rest. If any physical activity is conducted, discomfort increases. |
Other variables
Other variables with an impact on the primary outcome were also measured or obtained from the participants’ medical records and these included age, gender, BMI (height and weight), high blood pressure, diabetes status, posterior wall thickness and NYHA functional classification. Age and gender were obtained from the participants through the interviewer-based questionnaires. High blood pressure was defined as any blood pressure of 140/90 mmHg or higher, and this was obtained from the participants’ medical records. BMI was calculated using the participants’ height and weight and these were obtained from the participants’ medical records (BMI = weight (kg)/ Height (m2)). NYHA functional classification was assigned by the specialist physician based on the patients’ limitations during physical activity. Posterior wall thickness was defined as the thickness of the heart’s posterior walls and this was obtained from the echocardiography report. The normal range of the posterior wall thickness was considered as any values between 6 to 10 mm in male subjects and 6 to 9 mm in female subjects, and these were the ranges used at PGH.
NT-proBNP outcomes
Receiver operating characteristic (ROC) curves were produced from the NT-proBNP values in relation to the diagnosis of CHF. Diagnostic precision was determined by calculating the following:
Sensitivity
Sensitivity was defined as the ability of the NT-proBNP test to correctly designate an individual with CHF as having the disease. This was calculated using the formula shown in table 3.
Specificity
Specificity was defined as the ability of the NT-proBNP test to designate an individual without CHF as not having the disease. This was calculated using the formula shown in table 3.
Diagnostic accuracy
Diagnostic accuracy was defined as the ability of NT-proBNP to discriminate subjects with CHF from those who do not. This was done by comparing the NT-proBNP results with outcomes of the same subjects from the gold standard method.
Positive Predictive Value (PPV)
PPV was defined as the probability that a patient with an abnormally high NT-proBNP test result actually has CHF. This was calculated using the formula shown in table 3.
Negative Predictive Value (NPV)
NPV was defined as the probability that a person with a normal test result was truly free of CHF. In order to determine the PPV and NPV, a cut-off value was first established. This was calculated using the formula shown in table 3 below.
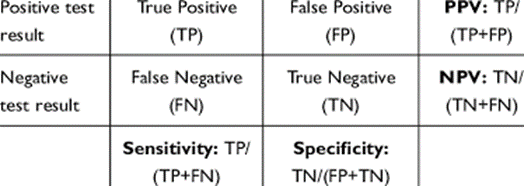
Table 3. Formulas for calculation of sensitivity, specificity, PPV and NPV.
Data Analysis and Organisation
Epi info 7 statistical software was used to capture and analyse data. Demographic, clinical, analytical and echocardiographic data were collected from each patient, introduced into a database, and analysed using the software. Individual participant data was first analysed separately before being reduced to aggregate data for statistical analysis. Descriptive statistics were used to describe the study population and presented as proportions, means, medians and inter-quartile range (IQR); these were generated by using the same statistical software. The Shapiro-Wilk test was used to test for normality. Level of significance was set at 5%.
Ethical Consideration
Ethical approval was sought from the Joint Research and Ethics Committee (JREC Ref: 280/2022). Permission was also sought from Parirenyatwa Group of Hospital authorities and these included the Clinical Director, the Matrons and Sisters in Charge at the respective medical wards.
Informed Consent
Written informed consent was obtained from all participants prior to sample collection. Participants incapable of reading and signing the written consent were assisted by either their relatives or sister in charge at that ward. Participants under the age of 18 were completely excluded from the study.
Voluntarism
Participation in this study was voluntary and this was clearly stated to the prospective participants prior to the study. Prospective research participants were fully informed about the procedures and risks involved in the study and they were asked to consent to participate. Participants were free to withdraw their consent and discontinue from participating in the study at any given time without being penalised.
Confidentiality
Participant information, records and results were treated with confidentiality. Password protected documents were used to ensure data security. Individual responses were not linked with participants’ identities and sample identifiers were only accessible to the researcher. The completed questionnaires were kept in files which were stored in lockable cupboards and these were only accessible to the researcher.
Risks and Benefits
All risks, discomforts, inconveniences and/ or benefits to the study participants were clearly explained to the potential participants before being enrolled into the study. Benefits to the general population or public health were also explained to the participants.
No foreseeable risks, discomforts or inconveniences were expected to be encountered by the participants in this study. The main benefit of the study to the participants was that they were going to have their NT-proBNP tests done for free and have the results which were going to assist their doctor in coming up with a suitable diagnosis. This study also helped the general population by determining whether NT-proBNP can be employed as a cheaper and alternative screening test for CHF.
DATA PRESENTATION, ANALYSIS AND INTERPRETATION
Demographic characteristics of the study population
A total of 110 patients with recent-onset dyspnoea of differing severity were enrolled into the study. All patients were hospitalised and admitted at PGH medical wards with suspected CHF. Variables were expressed as means± standard deviations (SD) if normally distributed, and median (IQR) if not normally distributed, unless otherwise stated. The ages of the study participants ranged from 56 years old to 85 years old, with a mean age of 71±7 years old. CHF was diagnosed in 74 (67.3%) of the participants, with the remaining 36 (32.7%) participants having dyspnoea due to non-cardiac causes. The ages of the patients with CHF were significantly higher than those of the patients with non-cardiac origin dyspnoea, with no difference with respect to sex. The weights of the participants ranged from 52.2 kg to 87.5 kg, with a mean weight of 68.2±70.1kg, and the heights ranged from 1.24m to 1.78m, with a median height of 1.59m (IQR 1.55-1.65). All participants were Africans and they all belonged to the Christianity denomination. Table 4 shows the demographic characteristics and semiologic findings in the study population.
Table 4. Demographic characteristics and semiologic findings in the study population
| All participants
(n = 110) |
CHF
(n = 74) |
Non-cardiac origin (n = 36) | p-value | |
| Age (years) | 71±7 | 74±6 | 64±5 | <0.001 |
| Gender
Males Females |
50 (45.5%) 60 (54.5%) |
37 (50%) 37 (50%) |
13 (36.1%) 23 (63.9%) |
0.170 |
| Body weight (kg) | 68.2±70.1 | 68.1±7.7 | 70.1±9.4 | 0.260 |
| Height (m) | 1.59 (1.55-1.65) | 1.59 (1.56-1.62) | 1.59 (1.52-1.67) | 0.888 |
| BMI
Median (IQR) |
27.37 (24.28-29.85) | 27.08 (24.11-29.82) | 27.83 (25.14-30.43) | 0.393 |
| High blood pressure
Yes No |
35 (31.8%) 75 (68.2%) |
22 (29.7%) 52 (70.3%) |
13 (36.1%) 23 (63.9%) |
0.810 |
| Diabetes
Yes No |
16 (14.5%) 94 (85.5%) |
11 (14.9%) 63 (85.1%) |
5 (13.9%) 31 (86.1%) |
0.660 |
| Posterior wall thickness (mm) | 10.4±3.3 | 10.4±3.5 | 10.3±3.1 | 0.538 |
Key: CHF, Congestive heart failure; BMI, Body mass index; NS, not significant.
Diagnoses, symptom severity, and echocardiography results
Dyspnoea was the most common symptom, 110 (100%), followed by shortness of breath, 60 (54.5%), arrythmias, 52 (47.3%), chest tightness or discomfort with exertion, 42 (38.2%), palpitations, 40 (36.4%), unreasonable breathlessness, 25 (22.7%), neck vein dislocation, 16 (14.5%), and orthopnoea, 12 (10.9%). Figure 5 shows the common symptoms among the study participants.
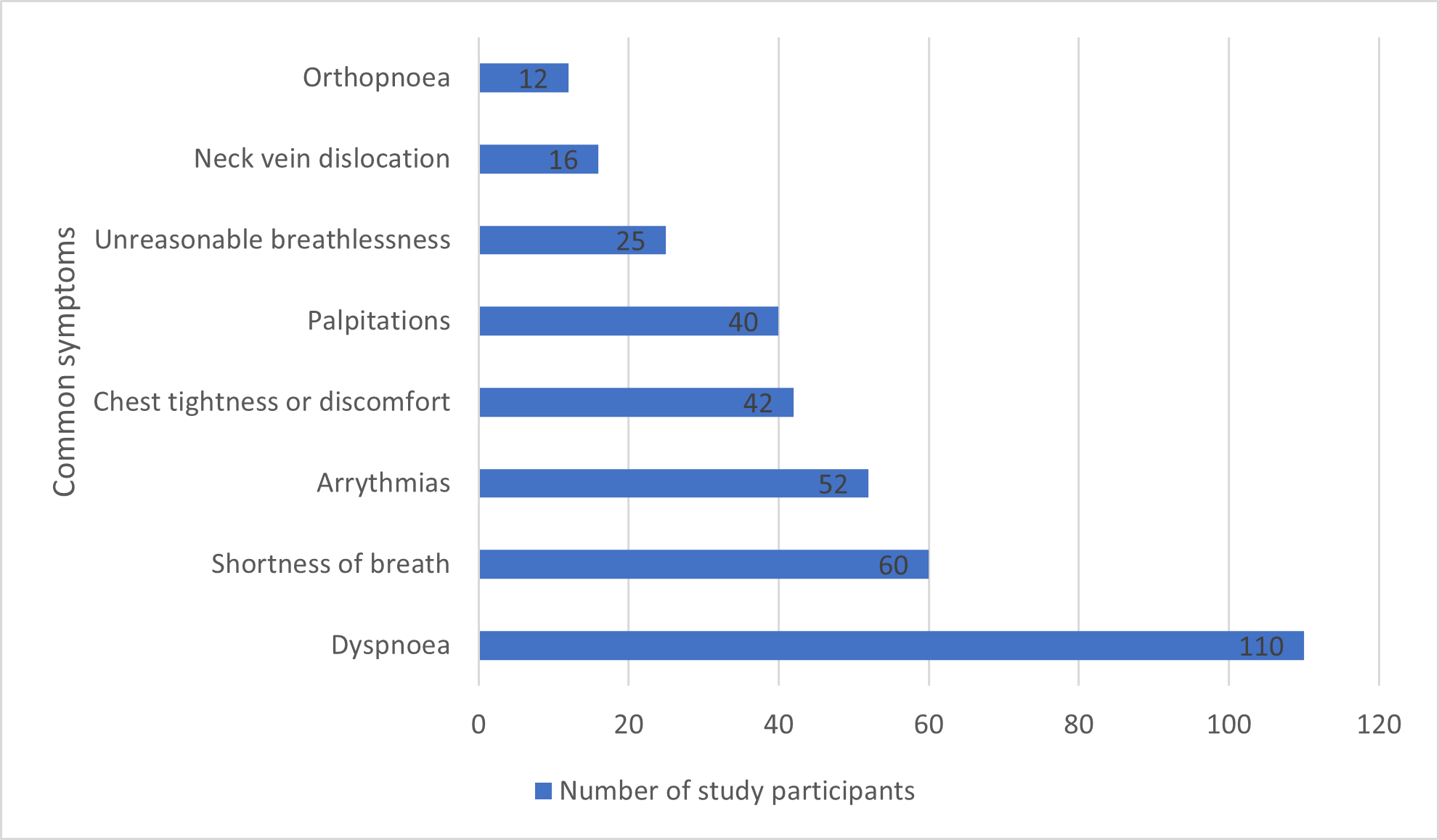
Figure 4. Common symptoms among the study participants
Based on symptom severity, all participants included belonged to NYHA functional classes II, III and IV. After a standard echocardiography, 74 (67.3%) of the study participants were found to have CHF whereas 36 (32.7%) had dyspnoea of non-cardiac origin, as shown in figure 6.
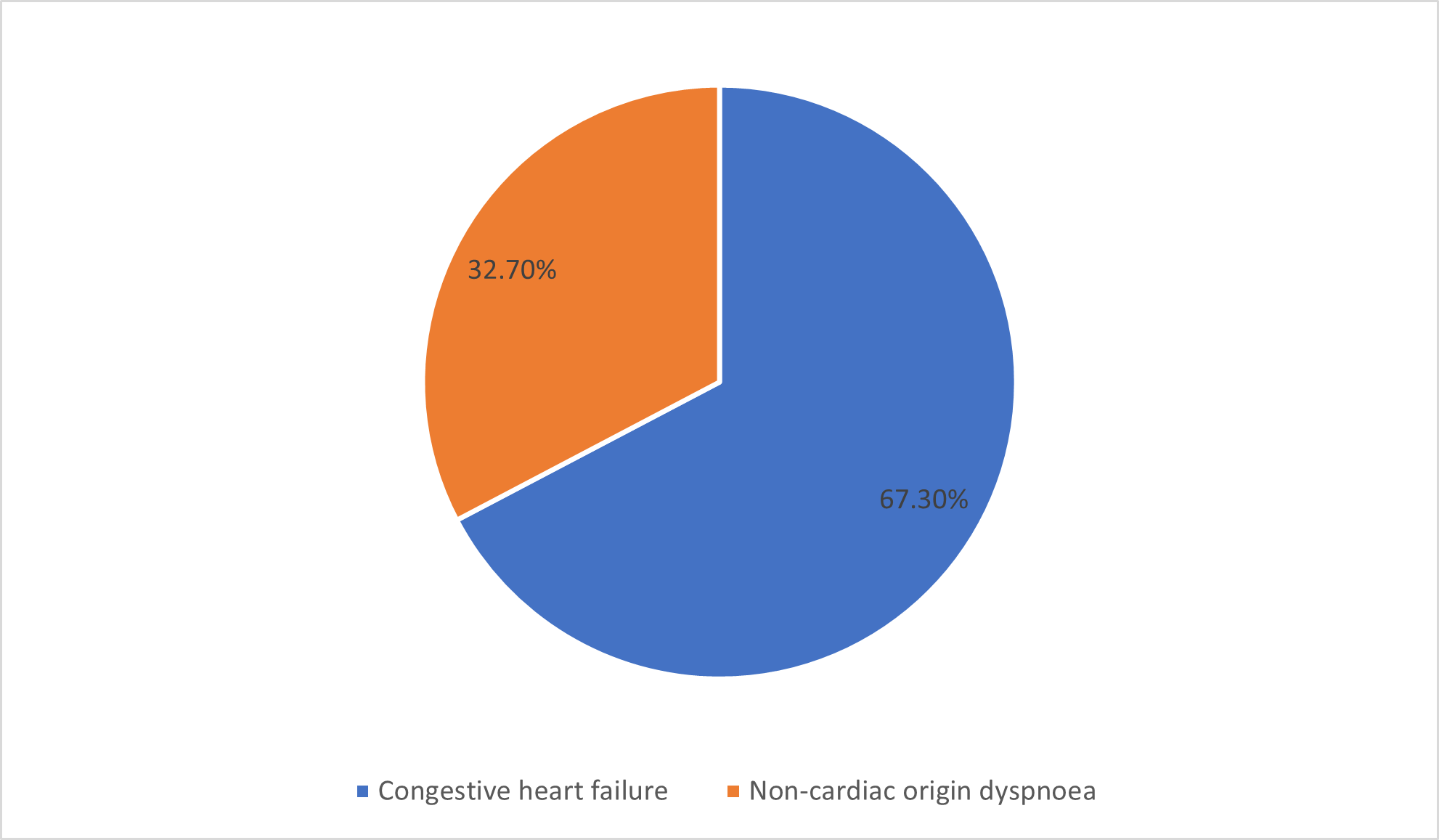
Figure 5. Distribution of CHF status by echocardiography
Among those with CHF, 35 (47.3%) fell in NYHA functional class II, 30 (40.5%) fell in class III, and 9 (12.2%) fell in class IV. Among those with non-cardiac origin dyspnoea, 32 (88.9%) fell in NYHA functional class II, 3 (8.3%) fell in class III, and 1 (2.8%) fell in class IV. Figure 7 shows the NYHA classification of the study population.
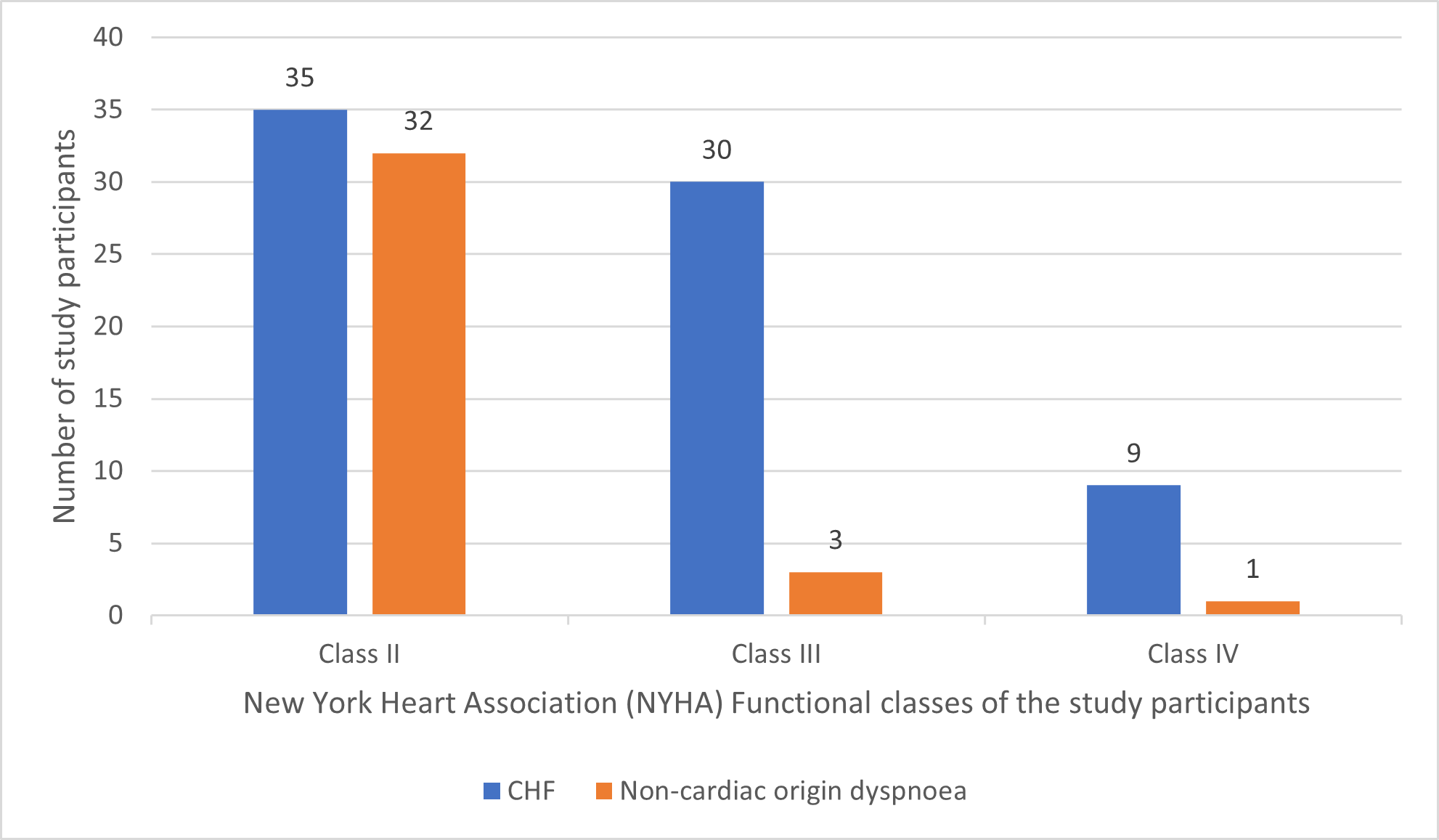
Figure 6. NYHA functional classification of the study population
Among the patients with CHF, 33 (44.6%) had a left ventricular ejection fraction (LVEF) of <40%, and these were classified as CHF patients with left ventricular dysfunction, and 41 (55.4%) had a LVEF of 40% or greater, and these were classified as CHF patients with preserved systolic function (Table 5). No significant differences were seen between the patient groups in terms of the thickness of the left ventricular wall.
Table 5. Echocardiographic findings of the study participants
| Condition | Parameter | All participants (n=110) | CHF patients (n=74) | Non-cardiac dyspnoeic patients (n=36) |
| Congestive heart failure with preserved systolic function | LVEF ≥40% | 77 (70.0%) | 41 (55.4%) | 36 (100%) |
| Congestive heart failure with left ventricular dysfunction | LVEF <40% | 33 (30.0%)
|
33 (44.6%)
|
0 (0%)
|
Key: LVEF, Left ventricular ejection fraction; CHF, Congestive heart failure.
Diagnostic usefulness of NT-proBNP levels in the diagnosis of CHF
Plasma NT-proBNP levels recorded were significantly higher in patients with CHF as compared to those with non-cardiac origin dyspnoea, P<0.001 (Table 6).
Table 6. Plasma NT-proBNP levels in patients with CHF and non-cardiac origin dyspnoea
| Echocardiography | Frequency | Percentage (%) | Median Plasma NT-proBNP (pg/ml) | IQR | p-value |
| Non-cardiac origin dyspnoea | 36 | 32.7 | 49.5 | 34.5-69.5 |
<0.001 |
| CHF | 74 | 67.3 | 492.5 | 300.0-709.0 | |
| Total | 110 | 100.0 | 300.5 | 70.0-597.0 |
Key: CHF, congestive heart failure; NT-proBNP, N-terminal pro-brain natriuretic peptide; IQR, Interquartile range.
Among the CHF patients, NT-proBNP levels significantly increased with NYHA functional class as shown in Table 7; P= 0.0001.
Table 7. Mean plasma NT-proBNP in patients with CHF according to the NYHA functional classification
| NYHA functional classification | Median plasma NT-proBNP (pg/ml) | IQR | p-value |
| II | 297 | 191-332 |
0.0001 |
| III | 612 | 501-742 | |
| IV | 3830 | 1444-9689 | |
| Overall | 492.5 | 300-709 |
Key: NYHA, New York Heart Association; NT-proBNP, N-terminal pro-brain natriuretic peptide; IQR, Interquartile range
CHF patients with impaired systolic function, as determined from the echocardiography results, had significantly higher NT-proBNP levels than those with CHF with preserved systolic function, P<0.001 (Table 8)
Table 8. Mean plasma NT-proBNP levels in patients with CHF according to the LVEF (above or below 40%).
| LVEF | Median plasma NT-proBNP (pg/ml) | IQR | p-value |
| <40% | 709 | 597-974 |
<0.001 |
| >40% | 301 | 196-401 | |
| Overall | 492 | 300-709 |
Key: LVEF, Left ventricular ejection fraction; NT-proBNP, N-terminal pro-brain natriuretic peptide; IQR, Interquartile range
Diagnostic performance characteristics of the NT-proBNP assay
Using a cut-off value of 100 pg/ml, NT-proBNP was found to have a sensitivity of 97.3%, a specificity of 91.7%, a PPV of 96.0% and a NPV of 94.3% in identifying CHF among patients suspected to have the disease. A full summary of the performance characteristics is shown in table 9. Any other cut-off value was not considered in this analysis because of the high sensitivity and reasonable specificity observed using the selected cut-off value.
Table 9. Sensitivity test results for plasma NT-proBNP
|
Echocardiography |
Plasma NT-proBNP |
Total |
|
| Positive (CHF) | Normal (Non-cardiac origin) | ||
| Abnormal (CHF) | 72 | 2 | 74 |
| Normal (Non-cardiac dyspnoea) | 3 | 33 | 36 |
| Total | 75 | 35 | 110 |
Key: CHF, Congestive heart failure; NT-proBNP, N-terminal pro-brain natriuretic peptide.
The Receiver Operating Characteristic (ROC) curve was plotted using sensitivity against 1-specificity values for the diagnostic value of NT-proBNP as shown in figure 8, and the total area under the ROC curve was 0.9448 (94.5%).
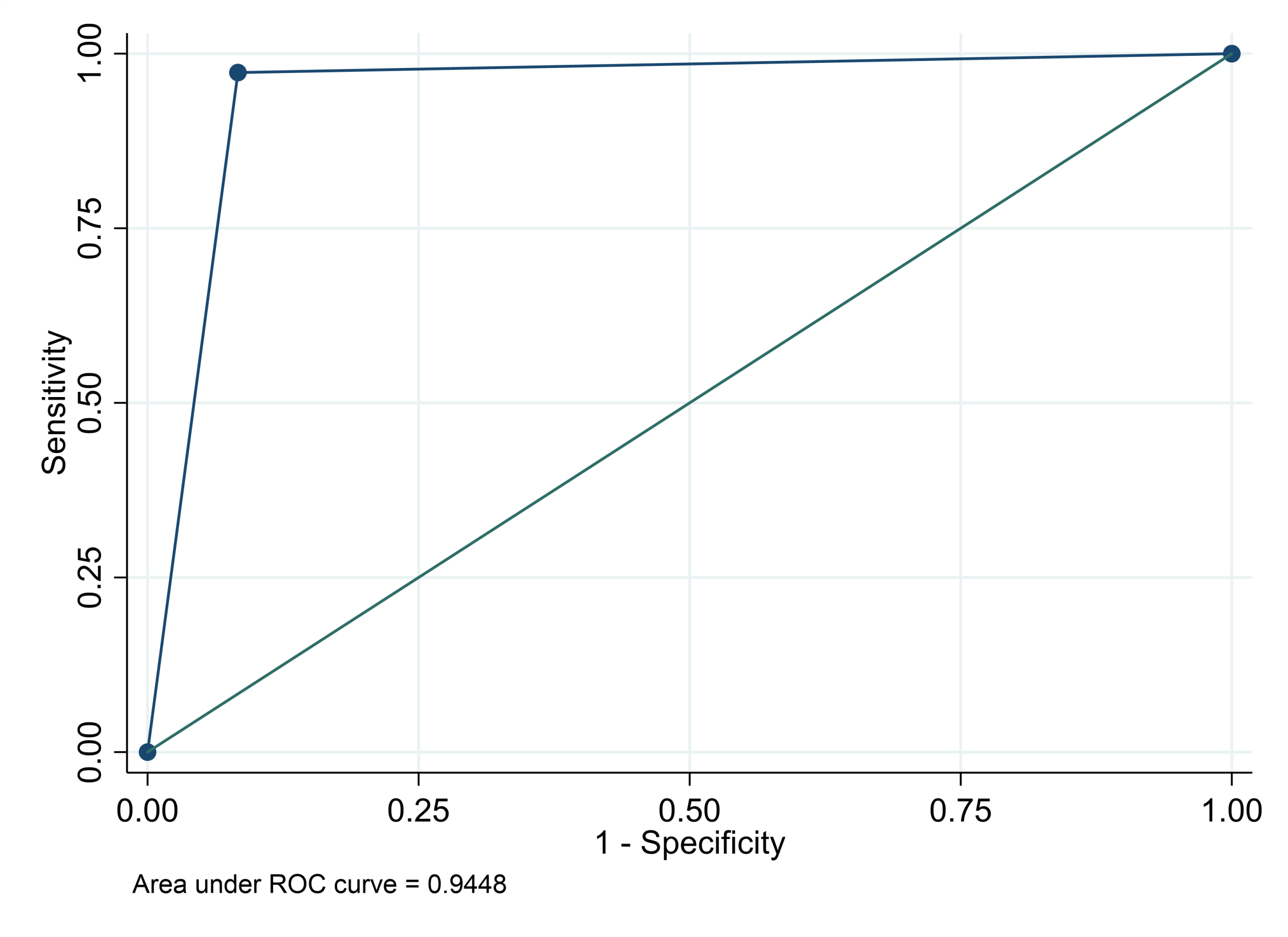
Figure 7. ROC curve for the diagnostic value of plasma NT-proBNP.
DISCUSSION, LIMITATIONS AND RECOMMENDATIONS
Discussion
The main aim of this study was to determine the diagnostic and therapeutic potential of NT-proBNP in the diagnosis of CHF in patients suspected to have the disease at PGH. Findings from the study demonstrated that the NT-proBNP test has a high sensitivity, specificity, PPV and NPV, suggesting that concentrations of NT-proBNP within appropriate cut-off points can rule out the presence of CHF in patients suspected to have the disease with a high degree of confidence.
A total of 110 patients with recent-onset dyspnoea were enrolled into the study, and 45.5% were males whilst 54.5% were females. The mean age was 71±7 years old. Using the echocardiography, as the gold standard screening method, 76 of the 110 patients were diagnosed with CHF and the remaining 34 had non-cardiac origin dyspnoea. Plasma NT-proBNP levels were also assayed for all the patients, and the levels were significantly higher in patients with CHF as compared to those with non-cardiac origin dyspnoea, P<0.001 (Table 6). This could be due to the fact that CHF is associated with cardiac dysfunction, which is characterised with complex neurohormonal responses which increase the circulatory levels of an array of plasma hormones including NT-proBNP. ProBNP is secreted into ventricles in response to volume expansion and pressure overload, and it breaks down into its two cleaved forms; NT-proBNP and BNP. CHF patients experience increased wall stretch due to volume and pressure overload and this leads to an increase in circulating natriuretic peptides, ANP and BNP, and their N-terminal fragments NT-proANP and NT-proBNP (65).
The ages of the patients were also significantly higher in CHF patients as compared to those with non-cardiac origin dyspnoea, P<0.001 (Table 4). Elderly patients tend to be more prone to a physical decline due to aging and poor cardiovascular management throughout life, and hence they are more prone to CHF as compared to their younger compatriots. This may also be related to a decline in myocardial function, myocardial fibrosis, cardiovascular stiffness and the reduction in clearance of NT-proBNP which is typical for senescence. Anguita et al. (66) reported increased levels of plasma NT-proBNP levels in patients with CHF as compared to those who had non-cardiac origin dyspnoea, and the ages of the patients were significantly higher in CHF patients as compared to their compatriots. These findings are consistent with findings from the current study. Several studies have also reported significant differences in plasma NT-proBNP levels amongst CHF patients in comparison to those with non-cardiac origin dyspnoea which is consistent with findings from the current study (4, 65, 67, 68, 69, 70, 71, 72, 73, 74). However, Sirithunyanont et al. (67) reported no significant differences in terms of the ages of the patients with CHF and those with non-cardiac origin dyspnoea, which is in contrast with findings from the current study.
No significant differences were seen in terms of gender, body weight, height, BMI, blood pressure and diabetes mellitus amongst the two groups of patients (Table 4). This is consistent with reports from some previous studies (66, 67, 74). Nayer et al. (7), Redfield et al. (69), Rorth et al. (70) and Palazzuoli et al. (73), all reported an inverse relationship between circulating natriuretic peptides and BMI which they attributed to the increased expression of natriuretic peptide clearance receptors by adipose tissue, resulting in increased clearance of natriuretic peptides in obese patients. However, these findings are in contrast with results from the current study which showed no relationship between circulating natriuretic peptides and BMI.
Close to half (44.6%) of the patients with CHF had left ventricular dysfunction whereas all of the patients with non-cardiac origin dyspnoea had preserved systolic function (Table 5). Plasma NT-proBNP levels were significantly increased in CHF patients with left ventricular dysfunction as compared to those with CHF with preserved systolic function, P<0.001 (Table 8). This ventricular dysfunction may also have significantly contributed to the increase in plasma NT-proBNP levels amongst patients with CHF. This is because increases in plasma ANP and BNP, and their amino-terminal congeners are related to cardiac structure and function (48) as evidenced by differences in plasma NT-proBNP levels amongst the two groups of participants. Similar findings were reported by Taylor et al. (74) in a study which investigated the potential role of NT-proBNP in screening for and predicting prognosis in heart failure, where all participants with heart failure had an ejection fraction of less than 40% and elevated NT-proBNP levels. Tschope et al. (77), in a study which investigated the role of NT-proBNP in the diagnostics of isolated diastolic dysfunction, reported significantly higher NT-proBNP levels in patients with impaired ventricular diastolic pattern, which further supported the findings in the current study. Since NT-proBNP production is related to cardiac structure and function, patients with left ventricular dysfunction are associated with increasing cardiac dysfunction hence the increased production of NT-proBNP. Anguita et al. (66), however, reported similar NT-proBNP values in patients with CHF and a LVEF of above or below 45%, findings which are in contrast with results from the current study.
Plasma NT-proBNP levels in patients with CHF increased with the severity of dyspnoea as indicated with the significant differences in plasma NT-proBNP levels amongst the different NYHA functional classes, P=0.0001 (Table 7). As the NYHA functional class increases so does the level of heart dysfunction and severity of the disease, and as mentioned earlier, increments in plasma NT-proBNP are related to cardiac structure and function (48, 65). These findings are consistent with results from several other previous studies (65, 78, 79, 80).
The area under the ROC curve in the present study was 0.9448. This is consistent with findings in the majority of other studies where the area under the ROC curve has been above 0.90 (78, 79, 80, 81, 82, 83, 84). However, contrasting results were reported by Anguita et al. (66), where the area under the ROC curve was 0.87±0.02, and Pascual et al. (85), where the area under the ROC curve was 0.72. The cut-off value in the current study was 100 pg/ml and this was associated with a negative predictive power of 94.3% which is also consistent with findings from other studies where the figure was greater than 90%, however, Anguita et al. (66) also reported a negative predictive power of 68%. A very high positive predictive power of 96% was reported in the present study and this means that, in a population with the characteristics of the present sample, nearly all (96%) of those who present at the emergency ward with NT-proBNP values greater than 100pg/ml have CHF.
Natriuretic peptides are already in use in some clinical practices to determine the likelihood of CHF and guide referrals for echocardiography, however, the optimal cut-off level is still unclear (74, 75, 76). There is need to come up with a universally accepted cut-off value that could permit plasma NT-proBNP assays to clinical practice in all settings. The National Institute for Health and Care Excellence (NICE) clinical guideline on the management of chronic heart failure recommends an NT-proBNP cut-off of 400 pg/ml to be used as the threshold to refer for echocardiography in symptomatic patients, whereas the European Society of Cardiology suggests a threshold of 125 pg/ml to exclude heart failure (74). Fuat et al. (86) reported a cut-off of 150 pg/ml as having an NPV of 92% in a primary care community heart failure clinic, in symptomatic patients. Data from the current study suggests that 100 pg/ml is a more reliable threshold for further investigation amongst the current study population, which is consistent with findings by Angermann and Erti (65).
Limitations of the study
Since data and sample collection was limited to Parirenyatwa Group of Hospitals, the study findings cannot be generalised to other geographical regions and districts in Zimbabwe. A large-scale study to investigate the diagnostic potential of plasma NT-proBNP in patients suspected to have CHF in Zimbabwe is therefore recommended, so that the results can be generalised to the whole country.
All participants (100%) in the present study were Africans and of the Christianity religion, which may not reflect the ethnic diversity of the Zimbabwean population. Plasma NT-proBNP levels may vary depending on ethnicity and religion hence a multicentred study with participants from differing ethnical groups and denominations is recommended. Daniels et al. (87) reported race as a factor which can influence plasma NT-proBNP levels. He went on to report that Hispanics and Blacks had higher levels of plasma NT-proBNP with respect to the Caucasian population (87). In light of these findings, it is therefore imperative to conduct a multicentred study involving patients from different religions and races.
Another limitation is the lack of a universally accepted cut-off value for plasma NT-proBNP. A universally accepted cut-off value would allow the assay to be used in clinical practice in all settings without differences in results interpretation.
Recommendations
A large-scale study to investigate the diagnostic potential of plasma NT-proBNP in patients suspected to have CHF in Zimbabwe is recommended, so that the results can be generalised to the whole country. A large-scale international analysis of NT-proBNP testing for evaluating patients with suspected CHF is recommended so that a universally agreed plasma NT-proBNP cut-off value is achieved. This will allow the test to be used routinely in all clinical practices without differences in result interpretation. Further studies may also be needed to check on the importance of age stratification on the diagnostic sensitivity and specificity of plasma NT-proBNP assay.
CONCLUSION
Findings from the current study demonstrates the importance of plasma NT-proBNP in the diagnosis and exclusion of CHF in dyspnoeic patients. Plasma NT-proBNP has proved to be an important biomarker which can be used to assess diagnosis and severity of CHF as well as to potentially guide therapy in CHF patients. It is a simple, inexpensive, useful and highly effective diagnostic test for CHF. Although echocardiography remains the gold standard method regarding the provision of detailed information on cardiac performance and structure, imaging data alone is not sufficient enough to identify patients with adverse CHF outcomes. An integrated approach which can combine laboratory assays with imaging and clinical presentation will greatly improve the diagnosis of CHF.
DISSEMINATION OF FINDINGS
The study findings or outcomes of the analysis will be submitted for publication following all appropriate research reporting guidelines. The study outcome information was also disseminated to the University of Zimbabwe Chemical Pathology Unit, University of Zimbabwe library, Parirenyatwa Group of Hospitals management, Parirenyatwa Group of Hospitals medical wards and to GoPath Clinical Laboratories.
Education 5.0 Innovation of the study
This study aims to support education 5.0 innovation by addressing the skills deficit through developing Zimbabwe’s knowledge. Currently, NT-proBNP is rarely or not requested at all at Parirenyatwa Group of Hospitals, and its introduction as a screening test will produce a relevant, competitive and cost-effective service which will contribute towards the modernization and industrialization of Zimbabwe.
ACKNOWLEDGEMENTS
I would like to profoundly thank the corresponding supervisor, Mr T Nyamayaro for his guidance, useful critiques, encouragement and support throughout the course of the research study. Special mention also goes to the Clinical Director of Parirenyatwa Group of Hospitals, the matrons and sisters in charge at Parirenyatwa Group of Hospitals medical wards for granting me the permission to carry out this study. I would also want to thank the sisters at the medical wards for their assistance during participant recruitment and enrolment, and GoPath Clinical Laboratories’ management and staff for allowing me to process my samples using their laboratory equipment and resources. I am also grateful to Mr Chikwasha for his timeous statistical data analysis and valuable guidance.
Finally, I would like to thank my wife, Gracious Chawasarira, for her encouragement and unwavering support throughout this research study.
ACRONYMS AND ABBREVIATIONS
ANP Atrial natriuretic peptide
BNP B-type natriuretic peptide
BMI Body Mass Index
CAD Coronary artery disease
cGMP cyclic Guanosine Monophosphate
CHF Congestive Heart Failure
CNP C-type natriuretic peptide
EDTA Ethylenediamine tetra acetic acid
ESC European Society for Cardiology
HF Heart Failure
IHD Ischemic Heart Disease
IQR Interquartile range
LVEF Left ventricular ejection fraction
NPR-A Natriuretic peptide receptor type A
NPR-C Natriuretic peptide receptor type C
NPV Negative Predictive Value
NT-proBNP N-Terminal pro B-type natriuretic peptide
NVD Neck vein distention
NYHA New York Heart Association
PPV Positive Predictive Value
PGH Parirenyatwa Group of Hospitals
US-FDA United States Food and Drug Administration
RAAS Renin-angiotensin-aldosterone system
SSA Sub-Saharan Africa
SNS Sympathetic Nervous System
REFERENCES
- Inamdar A.A, Inamdar A.C. Heart Failure: Diagnosis, Management and Utilization. Journal of Clinical Medicine. 2016; 5(7): 62. Available from: https://doi.org/10.3390/jcm50760062. Accessed on 03 January 2022.
- Castelnuovon A.D, Veronesi G, Costanzo S, Zeller T, Schnabel R.B, Curtis A, Salomaa V, Borchini R, Ferrario M, Giampaoli S, Kee F, Soderberg S, Niiranen T, Kuulasmaa K, Gaetano G, Donati M.B, Blankenberg S, Iacoviello L. NT-proBNP (N-Terminal Pro-B-Type Natriuretic Peptide) and the Risk of Stroke. Stroke. 2019; 50: 610-617.
- Maries L, Manitiu I. Diagnostic and prognostic values of B-type natriuretic peptides (BNP) and N-terminal fragment brain natriuretic peptides (NT-proBNP). Cardiovascular Journal of Africa. 2013; 24(7):286-289.
- Weber M, Hamm C. Role of B-type natriuretic peptide (BNP) and NT-proBNP in clinical routine. Heart. 2006; 92(6): 843-849.
- Balion C, Santaguida P.L, Hill S, Worster A, McQueen M, Oremus M, McKelvie R, Booker L, Fagbemi J, Reichert S, Raina P. Testing for BNP and NT-proBNP in the diagnosis and prognosis of heart failure. Evidence Report/ Technology Assessment. 2006; 142: 1-147.
- Suzuki S, Sugiyama S. The Molar ratio of N-terminal pro-B-type Natriuretic Peptide/ B-type Natriuretic Peptide for Heart Failure-related Events in Stable Outpatients with Cardiovascular Risk Factors. Internal Medicine. 2018; 57(18): 2621-2630.
- Nayer J, Aggarwal P, Galwankar S. Utility of point-of-care testing of natriuretic peptides (brain natriuretic peptide and n-terminal pro-brain natriuretic peptide) in the emergency department. International Journal of Critical Illness and Injury Science. 2014 Jul; 4(3): 209-15
- Costello-Boerrigter LC, Burnett JC Jr. The prognostic value of N-terminal pro B-type natriuretic peptide. Nature Clinical Practice Cardiovascular Medicine. 2005; 2: 194-201.
- Jarolim P. Serum biomarkers for heart failure. Cardiovascular Pathology. 2006; 15: 144-149.
- Dai Y, Yang J, Takagi A, Konishi H, Miyazaki T, Masuda H, et al. In-hospital and long-term outcomes of congestive heart failure: Predictive value of B-type and amino-terminal pro B-type natriuretic peptides and their ratio. Available from: https://doi.org/10.3892/etm.2017.4686
- Yancy C.W, Jessup M, Bozkurt B, Butler J, Casey D.E, Drazner M H, et al. ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of American College of Cardiology. 2013; 62(16): e147–e239.
- Malik A, Brito D, Vaqar S, Chhabra L. Congestive Heart Failure. StatPearls Publishing. Published November 7 2022.
- Dumitru L, Windle M.L, Sharma G.K. Heart Failure. Drugs and Diseases. Published in 2023.
- Fine N.M. Heart Failure (HF). Cardiovascular Disorders. Published/ Revised September 2022.
- Taylor K.S, Verbakel J.Y, Feakins B.G, Price C.P, Perera R, Bankhead C, Pluddermann A. Diagnostic accuracy of point-of-care natriuretic peptide testing for chronic heart failure in ambulatory care: systematic review and meta-analysis. British Medical Journal. 2018; 361: k1450. Available from: https://doi.org/10.1136/bmj.k1450
- Gallagher J, McDonald K, Ledwidge M, Watson C.J. Heart Failure in Sub-Saharan Africa. Cardiac Failure Review. 2018; 4(1): 21-24.
- Gtif I, Bonzid F, Charfeddine S, Abid L, Kharat N. Heart Failure disease: An African perspective. Archives of Cardiovascular Diseases. 2021;114(10): 680-690.
- Hertz J.T, Sakita A.T, Limkakeng A.T, Mmbaga B.T, Appiah L.T, Bartlett J.A, Galson S.W. The burden of acute coronary syndrome, heart failure and stroke among emergency department admissions in Tanzania: a retrospective observational study. African Journal of Emergency Medicine. 2019; 9: 180-184.
- Ayed H.B, Jemaa M.B, Trigui M, Hmida M.B, Kassis M, Jedidi J, Karray R, Abid L, Sourour Y, Damak J. Cardiovascular diseases in Southern Tunisia: current trends and future projections. Tunisia Medical Journal. 2019; 97(5): 659-666.
- Keates A.K, Mocumbi A.O, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: epidemiological profile and challenges. Nature Reviews Cardiology. 2017; 14: 273-293.
- Kraus S, Ogunbanjo G, Sliwa K, Ntusi N.A. Heart Failure in sub-Saharan Africa: A clinical approach. South African Medical Journal. 2016; 106: 23-31.
- Ntsekhe M, Damasceno A. Recent advances in the epidemiology, outcome, and prevention of myocardial infarction and stroke in sub-Saharan Africa. Heart. 2013; 99(17): 1230-1235.
- Hurst R.T, Ng D.W, Kendall C, Khandheria B. Clinical use of carotid intima-media thickness: review of the literature. Journal of the American Society of Echocardiography. 2007; 20(7): 907-914.
- Stein J. H, Korcarz C.E, Hurst R.T, Lonn E, Kendall C.B, Mohler E.R, Najjar S.S, Rembold C.M, Post W.S. Use of carotid ultrasound to identify subclinical vascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. Journal of the American Society of Echocardiography. 2008; 21(2): 93-111.
- Jeevarethinam A, Venuraju S, Weymouth M, Atwal S, Lahiri A. Carotid intimal thickness and plaque predict prevalence and severity of coronary atherosclerosis: a pilot study. Angiology. 2015; 66(1): 65-69.
- Ziembicka A.K, Tracz W, Przewlocki T, Pieniazek P, Sokolowski A, Konieczynska M. Association of increased carotid intima-media thickness with the extent of coronary artery disease. Heart. 2004; 90(11): 1286-1290.
- Sliwa K, Damasceno A, Mayosi B.M. Epidemiology and etiology of cardiomyopathy in Africa. Circulation. 2005; 112(23):3577-3583.
- Bloomfield G.S, Barasa F.A, Doll J.A, Velazquez E.J. Heart Failure in sub-Saharan Africa. Current Cardiology Reviews. 2013; 9(2): 157-173.
- Damasceno A, Mayosi B.M, Sani M, Ogah O.S, Mondo C, Ojji D, Dzudie A, Kouam C.K, Suliman A, Schrueder N, Yonga G, Ba S.A, Maru F, Alemayehu B, Edwards C, Davison B.A, Cotter G, Sliwa K. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries. Archives of Internal Medicine. 2012; 172(18): 1386-1394.
- Stewart S, Carrington M.J, Pretorius S, Ogah O.S, Blauwet L, Antras-Ferry J. Elevated risk factors but low burden of heart disease in urban African primary care patients: a fundamental role for primary prevention. International Journal of Cardiology. 2012; 158(2): 205-210.
- 2012 Population and Housing Census: Population Distribution by Administrative Areas, Tanzania National Bureau of Statistics, Dar es Salaam (2013).
- Sub-divisional projection for year 2016-2017 based on 2012 population and housing census. Dar es Salaam: Tanzania National Bureau of Statistics; 206.
- Wenban-Smith H. Population growth, internal migration and urbanization in Tanzania, 1967-2012. International Growth Centre. 2015.
- Owolabi M, Sarfo F, Howard V.J, Irvin M.R, Gebregziabher M, Akinyemi R, Bennett A, Armstrong K, Tiwari H.K, Akpalu A, Wahab K.W, Owolabi L, Fawale B, Komolafe M, Obiako R, Adebayo P, Manly J.M, Ogbole G, Melikam E, Laryea R, Saulson R, Jenkins C, Arnett D.K, Lackland D.T, Ovbiagele B, Howard G.Stroke in indigenous Africans, African Americans, and European Americans: interplay of racial and geographic factors. Stroke. 2017; 48(5): 1169-1175.
- Thrift A.G, Cadilhac D.A, Thayabaranathan T, Howard G, Howard V.J, Rothwell P.M, Donnan G.A. Global stroke statistics. International Journal of Stroke. 2014; 9(1): 6-18.
- National Clinical Guideline Centre. Chronic heart failure: national clinical guideline for diagnosis and management in primary and secondary care. National Clinical Guideline Centre, 2010.
- Ponikowski P, Voors A.A, Anker S.D, et al. Authors/ Task Force Members. Document Reviewers 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society for Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European Journal of Heart Failure. 2016; 18:891-975.
- Simons J.E, Don-Wauchope A.C. Evaluation of natriuretic peptide recommendations in heart failure clinical practice guidelines. Clinical Biochemistry. 2016: 49 (1-2):8–15.
- Maisel A, Hollander J E, Guss D, McCullough P, Nowak R, Green G, et al. Primary results of the Rapid Emergency Department Heart Failure Outpatient Trial (REDHOT). A multicentre study of B-type natriuretic peptide levels, emergency department decision making, and outcomes in patients presenting with shortness of breath. Journal of American College of Cardiology. 2004; 44(6):1328–1333.
- Murtagh G, Caniffe C, Mahgoub M, Blake L, McCarrol N, Crowley V, et al. Introduction of an NT-proBNP assay to an acute admission unit—A 2-year audit. European Journal of Internal Medicine. 2009; 20(1): 58–62. Available from: https://doi.org/10.1016/j.ejim.2008.04.021
- Bragazzi N.L, Zhong W, Shu J, Much A.A, Lotan D, Grupper A, Younis A, Dai H. Burden of heart failure and underlying causes in 195 coutries and territories from 1990 to 2017. European Journal of Preventive Cardiology. 2021; 28: 1682-190.
- Bozkurt B, Mann DL. Use of biomarkers in the management of heart failure: Are we there yet? Circulation. 2003; 107: 1231-1233.
- Jortani SA, Prabhu SD, Valdes R Jr. Strategies for developing biomarkers of heart failure, Clinical Chemistry. 2004; 50: 265-278.
- Harrison A, Amundson S. Evaluation and management of the acutely dyspneic patient: The role of biomarkers. American Journal of Emergency Medicine. 2005; 23: 371-378.
- Feinstein M.J, Hsue P.Y, Benjamin L, Bloomfield G.S, Currier J.S, Freiberg M.S, Grinspoon S.K, Levin J, Longenecker C.T, Post W.S. Characteristics, Prevention, and Management of Cardiovascular Disease in People Living With HIV: A Scientific Statement from the American Heart Association. Circulation. 20199; 140: e98-e124.
- Huet F, Nicoleau J, Dupuy A, Curinier C, Breuker C, Castet-Nicolas A, Lotierzo M, Kalmanovich E, Zerkowski L, Akodad M, Adda J, Agullo A, Leclercq F, Pasquie J.L, Battistella P, Roubille C, Fesler P, Mercier G, Bourel G, Cristol J.P, Roubille F. STADE-HF (sST2 As a help for management of HF): A pilot study. ESC Heart Failure. 2020; 7: 774-778.
- Aviles JM, Aviles RJ. Advances in cardiac biomarkers. Emergency Medicine Clinics of North America. 2005; 23: 959-975.
- Richards M, Troughton RW. NT-proBNP in heart failure: Therapeutic decisions and monitoring. European Journal of Heart Failure. 2004; 6: 351-354.
- Hayek S, Nemer M. Cardiac natriuretic peptides: From basic discovery to clinical practice. Cardiovascular Therapeutics. 2011; 29: 362-376.
- Valle R, Aspromonte N. Use of brain natriuretic peptide and bioimpedance to guide therapy in heart failure patients. Contributions to Nephrology. 2010; 164: 209-216.
- Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. The N-terminal pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. American Journal of Cardiology. 2005; 95: 948-54.
- Januzzi JL, van Kimmenade R, Lainchbury J, Bayes-Genis A, Ordonez-Llanos J, Santalo-Bel M, et al. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients: The International Collaborative of NT-proBNP Study. European Heart Journal. 2006; 27: 330-7.
- Onyemelukwe O.U, Oyati A.I, Danbauchi S.S, Obasohan A. B-Type Natriuretic Peptides (BNP) and Tissue Doppler E/e’ Before and After 4 Weeks Standard Treatment of African Heart Failure Subjects: The ABU-BNP Longitudinal Survey. Vascular Health and Risk Management. 2019; 15: 559-569.
- Sani M.U, Damasceno A, Davison B.A, Cotter G, Mayosi B.M, Edwards C, Azibani F, Adam T, Arif G, Jessen N, Sliwa K. N-terminal proBNP and galectin-3 are prognostic biomarkers of acute heart failure in sub-Saharan Africa: Lessons from the BAHEF trial. ESC Heart Failure. 2020; 8: 7-84.
- Badianyama M, Mpanya D, Adamu U, Sigauke F, Nel S, Tsabedze N. New Biomarkers and Their Potential Role in Heart Failure Treatment Optimisation- An African Perspective. Journal of Cardiovascular Development and Disease. 2022; 9(10): 335.
- McDonagh T.A, Metra M, Adamo M, Gardner R.S, Baumbach A, Bohm M, Burri H, Butler J, Celutkiene J, Chioncel O, Cleland J.G.F, Coats A.J.S, Crespo-Leiro M.G, Farmakis D, Gilard M, Heymans S, Hoes A.W, Jaarsma T, Jankowska E.A, Lainscak M, lam C.S.P, Lyon A.R, McMurray J.J.V, Mebazaa A, Mindham R, Muneretto C, Piepoli M.F, Price S, Rosano G.M.C, Ruschitzka F, Skibelund A.K. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journa. 2021; 42: 3599-3726.
- Heidenreich P.A, Bozkurt B, Aguilar D, Allen L.A, Byun J.J, Colvin M.M, Deswal M.H, Dunlay S.M, Evers L.R, 2022 AHA/ ACC/ HFSA Guidelines for the Management of Heart Failure. Journal of the American College of Cardiology. 2022; 79: e263-e421.
- Mant J, Doust J, Roalfe A, et al. Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care. Health Technology Assessment. 2009; 13:1-207.
- Zuber M, Cuculi F, Attenhofer Jost C H, et al. Value of brain natriuretic peptides in primary care patients with the clinical diagnosis of chronic heart failure. Scandinavian Cardiovascular Journal. 2009; 43:324-9.
- Maisel A. S. B-type natriuretic peptide (BNP)levels: diagnostic and therapeutic potential. Reviews in Cardiovascular Medicine. 2001; 2(2): S13-8.
- Bay M, Kirk V, Parner J, Hassager C, Nielsen H, Krogsgaard K, Trawinski J, Boegaard S, Aldershvile J. NT-proBNP: a new diagnostic screening tool to differentiate between patients with normal and reduced left ventricular systolic function. British Medical Journal. 2003; 89(2): 150-154.
- Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian Journal of Psychological Medicine. 2013; 35(2): 121-126.
- Bredy C, Ministeri M, Kempny A, Alonso-Gonzalez R, Swan L, Uebing A, Diller G.P, Gatzoulis M.A, Dimopoulos K. New York Heart Association (NYHA) classification in adults with congenital heart disease: relation to objective measures of exercise and outcome. European Journal- Quality of Care and Clinical Outcomes. 2018; 4(1): 51-58.
- Ontario Health (Quality). Use of B-Type Natriuretic Peptide (BNP) and N-Terminal proBNP (NT-proBNP) as Diagnostic Tests in Adults with suspected heart failure: A Health Technology Assessment. Ontario Health Technology Assessment Series. 2021; 21(2): 1-25.
- Angermann C.E, Erti G. Natriuretic peptides—new diagnostic markers in heart disease. Herz. 2004; 29(6): 609-17.
- Anguita M, Montes P, Jordan A, Casares G, Gomez I, Recio J, Martinez A, Zumalde J, Povar J, Ridocci F, Roig E, Batlle E. Utility of NT-proBNP for Diagnosing Heart Failure in a Heterogenous Population of Patients with Dyspnea. Spanish Multicenter Study. Revista Espanola de Cardiologia (English Edition). 2006; 59(5): 465-472
- Sirithunyanont C, Leowattana W, Sukumalchantra Y, Chaisupamonkollarp S, Watanawaroon S, Chivatanaporn B, Bhuripanyo K, Mahanonda N. Role of the plasma brain natriuretic peptide in differentiating patients with congestive heart failure from other diseases. Journal of the Medical Association of Thailand. 2003; 86(1): S87-95.
- Fonseca C, Sarmento P.M, Minez A, Goncalves E, Covas R, Dias A.R, Pina E.M.J, Ceia F. Comparative value of BNP and NT-proBNP in diagnosis of heart failure. Revista Portuguese de Cardiologia. 2004; 23(7-8): 979-91.
- Redfield M.M, Rodeheffer R.J, Jacobsen S.J, Mahoney D.W, Bailey K.R, Burnett Jr J.C. Plasma brain natriuretic peptide concentration: impact of age and gender. Journal of the American College of Cardiology. 2002; 40(5): 976-982.
- Rorth R, Jhund P.S, Yilmaz M.B, Kristensen S.L, Welsh P, Desai A.S, Kober L, Prescott M.T, Rouleau J.L, Solomon S.D, Swedberg K, Zile M.R, Packer M, McMurray J.V. Comparison of BNP and NT-proBNP in patients with Heart Failure and reduced Ejection Fraction. Circulation: Heart Failure. 2020. 13(2): e006541.
- Wieczorek S.J, Wu A.H, Christenson R, Krishnaswamy P, Gottlieb S, Rosano T, Hager D, Gardetto N, Chiu A, Bailly K. R, Maisel A. A rapid B-type natriuretic peptide assay accurately diagnoses left ventricular dysfunction and heart failure: a multicentre evaluation. American Heart Journal. 2002; 14(4): 834-839.
- Palazzuoli A, Gallotta M, Quatrini I, Nuti R. Natriuretic peptides (BNP and NT-proBNP): measurement and relevance in heart failure. Vascular Health and Risk Management. 2010; 6: 411-8.
- Palazzuoli A, Beltrami M, Ruocco G, Pellegrini M, Nuti R. The Role of Natriuretic Peptides for the Diagnosis of Left Ventricular Dysfunction. The Scientific World Journal. 2013; 784670.
- Taylor C.J, Roalfe A.K, IIes R, Hobbs F.D.R. The potential role of NT-proBNP in screening for and predicting prognosis in heart failure: a survival analysis. British Medical Journal Open. 2014; 4: e004675.
- The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure: European Society of Cardiology guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal. 2012; 33: 1787-847.
- National Institute of Health and Clinical Excellence. Chronic Heart Failure. Management of chronic heart failure in adults in primary and secondary care. National Institute for Health and Care Excellence. 2010.
- Tschope C, Kasner M, Westermann D, Gaub R, Poller W.C, Schultheiss H.P. The role of NT-proBNP in the diagnostics of isolated diastolic dysfunction: correlation with echocardiographic and invasive measurements. European Heart Journal. 2005; 26: 2277-84.
- Bayes-Genis A, Santalo M, Zapico E, Lopez L, Cotes C, Bellido J, Leta R, Casan P, Ordonez J. N-terminal probrain natriuretic peptide (NT-proBNP) in the emergency diagnosis and in-hospital monitoring of patients with dyspnoea and ventricular dysfunction. European Journal of Heart Failure. 2004; 6: 301-8.
- de Lemos J, McGuire D.K, Drazner M.H. B-type natriuretic peptide in cardiovascular disease. Lancet. 2003; 362: 316-22.
- Lainchbury J.G, Campbell E, Frampton C.M, Yandle T.G, Nicholls M.G, Richards A.M. Brain natriuretic peptide and N-terminal brain natriuretic peptide in the diagnosis of heart failure with acute shortness of breath. Journal of the American College of Cardiology. 2003; 42: 728-35.
- Bay M, Kirk J, Parner J, Hassager C, Nielsen H, Krogsgaard K, Trawinski J, Boesgaard S, Aldershvile J. NT-proBNP: a new diagnostic screening tool to differentiate between patients with normal and reduced left ventricular systolic function. Heart. 2003; 89: 150-4.
- McDonagh T.A, Holmer S, Raymond I, Luchner A, Hildebrandt P, Dargie H.J. NT-proBNP and the diagnosis of heart failure: a pooled analysis of three European epidemiological studies. European Journal of Heart Failure. 2004; 6: 269-74.
- Nielsen O.W, Kirk V, Bay M, Boesgaard S, Nielsen H. Value of N-terminal probrain natriuretic peptide in the elderly: data from the prospective Copenhagen Hospital Heart Failure study. European Journal of Heart Failure. 2004; 6: 275-80.
- Groenning B.A, Nilsson J.C, Sondergaard L, Pedersen F, Trawinski J, Baumann M, Larsson H.B.W, Hildebrandt P.R. Detection of left ventricular enlargement and impaired systolic function with plasma N-terminal pro brain natriuretic peptide concentrations. American Heart Journal. 2002; 143: 923-9.
- Pascual D.A, Cerdan M.C, Noguera J.A, Casas T, Munoz L, Garcia R, Ruiperez J.A, Martinez P, Valdes M. Usefulness of NT-proBNP in the Emergency Management of Patients with severe Dyspnoea and an uncertain Heart Failure diagnosis. Revista Espanola de Cardiologia. 2005; 58(10): 1155-1161.
- Fuat A, Murphy J.J, Hungin A.P, Curry J, Mehrzad A.A, Hetherington A, Johnston J.I, Smellie W.S.A, Duffy V, Cawley P. The diagnostic accuracy and utility of a B-type natriuretic peptide test in a community population of patients with suspected heart failure. British Journal of General Practice. 2006; 56: 327-33.
- Daniels L.B, Bhalla V, Clopton P, Hollander J.E, Guss D, McCullough P.A, Nowak R, Green G, Saltzberg M, Ellison S.R, Bhalla M.A, Jesse R, Maisel A. B-type natriuretic peptide (BNP) levels and ethnic disparities in perceived severity of heart failure. Results from the rapid emergency department heart failure outpatient trial (REDHOT) multicentre study of BNP levels and emergency department decision making in patients presenting with shortness of breath. Journal of Cardiac Failure. 2006; 12(4): 281-285.