
Factors Associated with the High Expiry Rate of Pharmaceutical Products within the Supply Chain in the Ministry of Health: A Case Stud of Choma District of Southern Province.
- Bupe Bwalya
- Bupe Getrude Mutono-Mwanza
- 5711-5736
- Aug 22, 2025
- Supply Chain Management
Factors Associated with the High Expiry Rate of Pharmaceutical Products within the Supply Chain in the Ministry of Health: A Case Study of Choma District of Southern Province.
Bupe Bwalya, Bupe Getrude Mutono-Mwanza
Graduate School of Business, University of Zambia, Lusaka, Zambia
*Corresponding Author
DOI: https://dx.doi.org/10.47772/IJRISS.2025.907000460
Received: 10 July 2025; Accepted: 18 July 2025; Published: 22 August 2025
ABSTRACT
Access to important drugs remains a major concern in many health-care systems, especially in developing countries. This study looked into the factors that contribute to high pharmaceutical expiry rates within the Ministry of Health’s supply chain in Choma District, Southern Province, Zambia. A cross-sectional quantitative approach based on Inventory Control Theory, Rational Choice Theory, and Resource-Based Theory was utilised to investigate operational, workforce, and donor-related factors impacting medicine wastage. Data were collected from 23 healthcare personnel at various sites. The results showed that 78.3% of all medicines in stock had expired, with critical medicines at 56.5%, donated drugs at 65.2%, and family planning items at 8.7%. Although 73.9% of respondents had more than two years of experience and 82.6% were involved in medicine management decisions, there was no significant link between these factors and expiry rates. Furthermore, 82.6% of respondents assessed their inventory knowledge as “very good” or “excellent,” although significant expiry rates remained. System-level variables surfaced as critical: 56.5% of institutions received donor stock that was close to expiration, 65.2% reported poor donor coordination, and only 17.4% employed real-time inventory management systems—despite the fact that 88.9% of those without such tools reported expired stock. While 91.3% claimed to have adequate storage infrastructure, qualitative feedback revealed that 8.7% of facilities stored medicines in non-compliant areas such as office spaces. According to the study, medicine expiration is primarily caused by supply chain inefficiencies, logistical misalignments, insufficient cold-chain infrastructure, and lax enforcement of procurement and storage protocols. Individual worker characteristics had a minimal impact. To reduce waste and increase pharmaceutical sustainability, the report suggests implementing automated inventory systems, strengthening donor coordinating frameworks, improving facility infrastructure, and enforcing standard operating procedures throughout Zambia’s public health sector.
Keywords: Pharmaceutical product expiry, healthcare outcomes, health worker concerns, cold-chain management, logistical challenges, and regulatory framework.
INTRODUCTION
The pharmaceutical supply chain is a vital component of global healthcare systems, enabling patients’ access to essential medicines (World Health Organisation, 2019). However, the supply chain faces various obstacles, including high expiry rates of pharmaceutical products, which cause compromises. The situation is considerably worse in certain of Africa’s and Asia’s lowest-income countries, where more than half of the population lacks regular access to crucial medicines (Kapoor 2018). Wastage is one of the reasons why medicines are so difficult to obtain. Medicines account for a considerable element of the healthcare system. The World Health Organisation (WHO) recognises access to safe and appropriate medications as a foundational component of the public health system (Manyazewal, 2020). This includes the delivery of health services that are linked to the provision of medicines, vaccinations, and medical breakthroughs that do not endanger patients (WHO, 2010). The requirement for such high-quality pharmaceuticals is embedded in Zambia’s health policy/constitution, where the government spends approximately 14 USD per capita on its citizens’ health (WHO, 2019). This allocation, while small, is larger than that of other developing nations such as the Central African Republic, the Democratic Republic of the Congo, Madagascar, and Niger (WHO, 2019). Although the amount to which this fraction is spent on medicines is unknown, this allocation alone implies that governments spend very little on the acquisition of vital medicines, with the remaining proportion procured by donors and out of pocket.
The majority of Zambians are willing to pay health-related insurance charges, such as National Health Insurance Management (NHIMA) (MOH, 2021). On the other hand, research has argued that higher out-of-pocket expenditure on essential medicines, particularly in developing countries such as Zambia, could indicate one of two things: a higher prevalence of multimorbidities in a population, or a lack of access to medical insurance. Similarly, it would imply limited supply of drugs in public health facilities, resulting in high prices (Sum et al., 2018).
However, the rate at which drugs expire in health institutions is cause for serious concern, exposing patients to preventable health hazards. According to a report released by the National Assembly Audit Committee 20201, approximately k8 million (800,000 USD) in medications expired in Zambia between 2007 and 2019. Relying on such compromised healthcare systems increased the burden on patients and customers from preventable health issues such as malaria and respiratory infections. It also compels consumers to pay more for medical expenditures in the private sector at the price of basic necessities.
Zambian public health facilities, particularly in Choma and Lusaka, are undersupplied with pharmaceuticals, and patients are frequently forced to purchase medications given in public health facilities from private pharmacies (Mushiba, 2020). However, a study in Pakistan found that outdated pharmaceuticals from the public healthcare system are common in private retailers (Bashaar et al., 2017). According to Mathew and J Other (2018), study findings have highlighted the necessity for health workers (pharmacists, nurses, and others) to understand medicines inventory management in order to reduce drug expiration (Mathew & John, 2013). According to the Auditor General’s report from 2016, various drugs such as antiretroviral drugs (ARVs), laboratory reagents, tuberculosis (TB), and malaria drugs worth K66, 801, 022, involving one thousand seven hundred and sixty-three (1,763) transactions, were kept at a rented warehouse in Makeni, Lusaka, and had expired. It further said that nine (9) health facilities surrendered medications and other medical supplies totalling K 943, 889.00 to Medical Stores Limited due to their short shelf life (National Assembly of Zambia, 2022). Zambia’s pharmaceutical supply chain is characterised by inadequate infrastructure, insufficient finance, and poor management practices, resulting in high product expiry rates (Zambia Ministry of Health, 2020). This problem is not new; it has been for decades. Previous audit reports of the Auditor-General for the finances included substantial volumes of expired drugs. As such, the purpose of this study was to identify factors related with the high expiry rate of pharmaceutical items throughout the Ministry of Health’s supply chain, with a focus on the Choma District in Zambia’s Southern Province.
LITERATURE REVIEW
An Overview of Zambia’s Pharmaceutical Industry
Zambia’s pharmaceutical business is significantly reliant on imported medications, particularly from India, due to local production constraints and regulatory barriers (Chongo and Chituta, 221). The sector faces issues including as medicine shortages and a lack of key supplies during pandemics, emphasising the need for better local production capacities. The Zambia Medicines and Medical Supplies Agency (ZAMMSA) has launched steps to improve storage capacity and distribution infrastructure, with the goal of strengthening the supply chain management system. However, Zambia lacks in innovation and R&D, impeding collaboration with the pharmaceutical industry for product scaling and commercialisation (Chonga and Chituta, 2021; UNDP, 2021; Zambia Association of Manufacturers, 2021). This assessment reveals that, while Zambia’s pharmaceutical industry confronts substantial obstacles, initiatives are underway to strengthen the supply chain and increase local production capabilities. As a result, implementing improved inventory management procedures, strengthening supply chain control, improving storage conditions, and establishing clear regulations for the disposal of outdated medicines are essential steps towards minimising pharmaceutical product expiry rates.
Zambian Ministry of Health Inventory Management Protocol and WHO Guidelines for Managing Pharmaceutical Supplies
The Zambian Ministry of Health (MoH) has created a comprehensive inventory management protocol to ensure the correctness and reliability of medical equipment utilised in the country. This procedure emphasises the necessity of equipment calibration, regular site inspections, staff training, and strategic data management. The MoH’s approach is intended to ensure high quality assurance and operational efficiency in the healthcare industry (Ministry of Health, Zambia, 2022).
In contrast, the World Health Organisation (WHO) offers comprehensive guidelines for managing pharmaceutical supplies that encompass a broader range of supply chain operations. These standards include procurement, purchasing, storage, distribution, transportation, repackaging, relabeling, documentation, and record-keeping procedures. The WHO recommendations are intended to ensure the quality and authenticity of pharmaceutical goods throughout the distribution chain, therefore protecting public health (World Health Organisation, 2010).
When the two are compared, it is clear that the Zambian Ministry of Health and the World Health Organisation priorities quality assurance and operational efficiency. However, the Zambian protocol is mainly concerned with the calibration and maintenance of medical equipment, whereas the WHO recommendations give a more complete framework for regulating the entire pharmaceutical supply chain. This distinction emphasises the importance of a specialised strategy to inventory management that addresses each country’s unique demands and challenges.
To assess the efficacy of these principles, investigate their impact on the efficiency and effectiveness of the pharmaceutical supply chain. The Zambian Ministry of Health’s protocol, which emphasises equipment calibration and staff training, has the potential to increase medical equipment accuracy and reliability. On the other hand, the WHO’s comprehensive guidelines ensure that all areas of the supply chain are addressed, potentially lowering the possibility of counterfeit and inferior products reaching the market. It was thus discovered that, while both the Zambian Ministry of Health’s inventory management protocol and the World Health Organization’s standards for managing pharmaceutical supplies strive to improve the quality and reliability of healthcare services, their scope and focus differ. A comparative review of these documents highlights each approach’s strengths and flaws, giving useful insights for improving national and global pharmaceutical supply chain regulations.
Pharmaceutical supply policies are critical to assuring the availability, price, and quality of medications and health goods. These regulations cover a wide range of activities, including procurement, distribution, storage, and inventory management. Effective pharmaceutical supply strategies are critical for maintaining a stable supply chain and ensuring patients’ access to critical medications (Management Sciences for Health, 2012).
Procurement is an important part of pharmaceutical supply management policies. Procurement refers to the process of procuring medications and health supplies from manufacturers or suppliers. Transparent and effective procurement practices are critical for ensuring that high-quality products are obtained at reasonable prices. This can include competitive bidding, supplier prequalification, and the application of international quality assurance standards (Management Sciences for Health, 2012).
Another key consideration is distribution. Distribution strategies ensure that medications arrive at their intended locations in a timely and efficient manner. This includes developing dependable transportation networks, ensuring suitable storage conditions, and deploying tracking technologies to monitor product movement. Effective distribution plans help to avoid stockouts and ensure that medications are available when and where they are required (World Health Organisation, 2024).
Storage and inventory management are also important aspects of pharmaceutical supply regulations. Proper storage conditions are required to ensure the quality and efficacy of medications. This includes managing temperature, humidity, and other environmental conditions that can impact pharmaceutical product stability. Inventory management entails monitoring stock levels, estimating demand, and applying reordering mechanisms to avoid overstocking or stockouts (Management Sciences for Health, 2012).
Pharmaceutical supply policies address not just operational aspects, but also regulatory and legal frameworks. These frameworks define regulations and standards for the manufacture, distribution, and sale of medications. They ensure that pharmaceutical products fulfil safety and efficacy requirements, and that counterfeit or substandard medications do not enter the market (World Health Organisation, 2024).
Overall, effective pharmaceutical supply regulations are critical for guaranteeing patients’ access to safe, effective, and inexpensive medications. These policies, which focus on procurement, distribution, storage, and regulatory frameworks, contribute to the maintenance of a stable and reliable supply chain that satisfies the demands of both healthcare professionals and patients.
Global Perspective on Medicine Supply and Pharmaceutical Product Expiration in Health Facilities
Many experts throughout the world have discovered that drug shortages can emerge when raw material supplies are disrupted. There could be a shortage of active pharmaceutical ingredients (API), excipients, or packaging materials (Dill and Ahn, 2014). Other studies show that India and China are key active pharmaceutical component suppliers at practically every economic level. Raw resources may be unavailable owing to political unrest, violent conflicts, animal sickness, trade disputes, environmental conditions, deterioration during transport, or low plant yield as a supply of material from the source country (Ventola, 2011; Coustasse et al., 2020). For example, Hurricane George in Puerto Rico caused drug shortages in 1998 (Gu et al., 2011; Rinaldi et al., 2017), and during the COVID-19 pandemic, active pharmaceutical ingredients (APIs), excipients, and pharmaceuticals were in low supply worldwide. As a result, the countries producing APIs (India, China, and the United States) ceased selling some APIs to other countries, resulting in a global medicine shortage. Furthermore, many other obstacles exist, such as a lack of packing material, disruptions in transportation, delayed shipping, delayed customer clearance, and restrictions on the import-export of APIs and pharmaceuticals around the world (Ayati et al., 2020; Badreldin and Atallah, 2021).
Furthermore, during the COVID-19 pandemic, API shortages were reported in the United States (Coustasse et al., 2020). When a single supplier provides the API and excipients for a medication, any supplier issues may result in a medicine shortage (Ventola, 2011). As a result, a product having at least three material sources is generally regarded as desirable (Hedman, 2016). Raw material scarcity was a major cause of medicine shortages. In high-income countries, medicine shortages are common due to business difficulties. Low market prices are the primary source of generics shortages. High-income countries have adopted the Beveridge Model (Spain, New Zealand, Cuba, Hong Kong), the Bismarck Model (Germany, France, Belgium, the Netherlands, Latin America), and the National Health Insurance Model (Canada, South Korea, Taiwan), which exempts patients from out-of-pocket expenses. However, in intermediate and low-income nations (remote areas of China, India, Africa, and South America), the Out-of-Pocket Model is effective, putting a strain on patients (Kos, 2019).
Furthermore, research in low and middle-income countries, such as Kenya, Fiji, Pakistan, and Sub-Saharan Africa, identified procurement processes as drivers of shortages (Malik et al., 2013; Walker et al., 2017). However, other researchers argue that few studies have been conducted in low and middle-income countries, with only increased out-of-pocket expenses reported as the economic impact of drug shortages (Fatima and Khaliq, 2017; Walker et al., 2017; Acosta et al., 2019). It has been observed that managing medicines shortages is heavily reliant on the health-care system, which includes a well-managed drug supply chain and an adopted health-care model.
Africa’s perspective on drug supplies and the expiration of pharmaceutical products at health institutions.
Studies have revealed that there is a difficulty of the vast volume of expired medicines accumulates worldwide due to over-prescription, mixed with overproduction of medicines Alnahas et al (2020). The majority of items are distributed to pharmacies and expire in 1 to 5 years from the date of manufacturing, with the exception of pharmaceuticals stored in temporary, provisional warehouses such as emergency settings. However, it is difficult to rely on the mentioned expiry date because medications cannot be used after their expiration date. As a result, the expiration date we observe may not correspond to the drug’s actual shelf life.
Tull (2018) verifies that Kenyan police thwarted a drug repackaging scheme in April 2018, according to media sources. In just one year, the Kenya Medical Supplies Authority lost Sh352 million (US$3.47 million) in pharmaceuticals owing to expiration or damage. The 2016/17 KEMSA report failed to explain expired stocking drugs, resulting in unnecessary loss to the authority when numerous hospitals complained of a drug shortage. In Uganda, a cross-sectional study of six public and 32 private medicine outlets in Kampala and Entebbe municipality revealed that drugs and medicines that are rapidly expiring include those for vertical programs, donated drugs, and those used at the lowest rate.
According to research, budgets allocated to medicines in developing countries are always high, and they are even the second most expensive category after human resources. As a result, proponents of this theory believe that the supply chain must be improved and sustained to prevent any loss, including pilferage, misuse, and expiry. As a result, the quality of care offered to patients suffers, and people lose faith in their healthcare system. This is mirrored in Rwanda’s instance, as documented by USAID-DELIVER Final Report 2016, which found that for many years, Rwanda’s medicine supply chain was inefficient due to insufficient quantification. The Final Report 2016 identifies interruptions in Rwanda’s health commodities supply chain and their implications for the government’s health goals. According to the survey, the Rwandan government and stakeholders are developing new supply chain management strategies to improve efficiency. Researchers emphasise the significance of a strong supply chain in assuring the availability of critical health commodities and reducing pharmaceutical expiration. Issues may arise with medicine selection, procurement, storage, distribution, and policies.
Zambian Perspective on Medicine Supply and Pharmaceutical Product Expiration in Health Facilities.
Cameron et al. (2009) claim that Zambia has a three-tier public sector distribution system for vital pharmaceuticals. Medical Stores Limited (MSL), a parastatal entity, manages the primary delivery of pharmaceuticals and other health commodities from Lusaka to around 120 district stores and hospitals. Secondary distribution of goods from district stores to about 1500 health facilities is the responsibility of District Health Management Teams (DHMTs), which report to the Ministry of Health. Despite increased investment in the procurement of vital drugs, their availability in health institutions remains severely low in many low- and middle-income nations. The lack of a well-functioning supply chain for important medicines is frequently the source of this low availability.
According to Heath (2019), a study was undertaken utilising a randomised trial in 439 health facilities and 24 districts in Zambia to better understand the ideal supply chain topology for vital medications distribution in the public sector of low-income nations. According to one study, a direct delivery system decreases stockouts of important drugs much more than typical multi-level systems. The direct flow of demand data from health facilities to the central supply agency enhances accountability and decision-making. However, system redesigns face difficulties in negotiating the political economy of the healthcare system. Efficient supply chains are critical for guaranteeing availability to life-saving pharmaceuticals, but comprehensive analysis of distribution networks and their impact on stockout rates is lacking. Many developing countries, like Zambia, have multi-level distribution systems, although the optimal number of levels remains unknown due to complex incentives. As health systems evolve, deciding between centralisation and decentralisation in supply chains becomes increasingly critical. Additional research is needed to determine the impact and cost effectiveness of system redesigns on supply chain performance. Strong political commitment and legislative action, backed up by rigorous evidence, are required to increase supply chain efficiency and accountability. Despite advancements in the medication procurement system, Zambian health centres continue to face shortages of key medicines. A 2006 survey discovered significant shortages of life-saving medications.
An empirical review of the research on the factors linked with drug and supply expiration. Factors linked with medicines and supplies expire in healthcare institutions. Knowledge and application of First Expiry First Out (FEFO); FEFO is a stock rotation approach that ensures that medicines with the earliest expiry date are used first, whereas First In First Out (FIFO) focusses on using stock that was received first, regardless of expiry date. The consequences of misunderstanding the two words (FEFO vs. FIFO) could result in medicines expiring.
Celeste Sauls (2016) conducted a study on “Trend in revenue loss due to expired medication at a large urban hospital in Johannesburg, South Africa” and discovered that, while the majority of participants claimed to know what the acronym meant, nearly half explained FEFO using First in First Out (FIFO) principles. Although respondents were aware of the acronym, their understanding was inaccurate, albeit the end result may have been the same. Medicines that were obtained initially may expire first and can be utilised before they do. This may differ from respondents knowing exactly what to do but being unable to put it into effect due to restrictions or practical obstacles.
Other research has found that inadequate medicine quantification, failure to follow donation standards, and a lack of stock management knowledge among health staff are some of the causes of medicine expiration in health facilities (Romero, 2013). In many cases, drugs are pushed to institutions regardless of their need, resulting in expiration (Tumwine et al., 2010).
The Malaysian Ministry of Health’s instructions for the usage of high alert medication recommended that all personnel thoroughly read the High Alert Medication labels before storing to ensure medications are maintained in the proper location. All High Alert Medications should be stored in individually marked containers (MoH, 2011). Whenever feasible, keep look-alike and sound-alike drugs, as well as different strengths of the same medicine, separate. The rules clearly stated that not employing TALL man writing to emphasise distinctions in prescription names, such as DOPamine and DOBUTamine, causes misunderstanding and may result in the expiration of pharmaceutical items.
Similarly, the Malaysian Pharmaceutical Services Guidelines on the Safe Use of High Alert Medications advised the use of standardised formats for written orders of cytotoxic drugs and parenteral feeding. Otherwise, if healthcare personnel and dispensers utilise acronyms when prescribing High Alert Medications, the medicines may be overlooked and end up on the shelf undispensed (MoH, 2011). Thus, for High Alert Medications administered, the dose, route, and rate of infusion must be specified, such as IV Dopamine 5mcg/kg over 1 minute. Other examples include prescription oral liquid drugs in milligrammes and avoiding using a trailing zero when prescribing 5.0 mg (otherwise, it can be misinterpreted as 50 mg).
Celeste Sauls (2016) conducted a study in South Africa and discovered that, according to hospital Standard Operating Procedures (SOPs), the pharmaceutical storage area must be under the authority of the responsible chemist and medicines must be delivered directly to the pharmacy. However, it was discovered that the chemist in charge was not always there, so different staff members were assigned to unpack and store medications. The department determines who these staff members are, as well as how drugs are received and stored. The SOP also advised someone to always be present to receive drugs and guarantee their proper packing and storage. At this facility, a “Ward Medicine Champion” and chemist’s assistant are appointed to execute this job. Observations revealed that, in some circumstances, the person in charge of packing the stock failed to verify the amount of products received in proportion to the orders placed. Furthermore, in certain cases, the identical things were ordered again with the next order placed by the ward, Celeste Sauls (2016).
Medicines that are presented, packed, and labelled in a language that is not widely known by health professionals in the country may expire since it is difficult to check the expiration date (1). Because donations come from several countries, the labelling of drugs may not be consistent with the required standards in the country. This also offers issues that can contribute to medications expiring while being stored because other medical workers may not be aware of the exact date when the medicines will expire, and medicine may not be issued in accordance with FEFO. During the tsunami in Indonesia, 60% of the gifts received were not on the country’s list of critical medicines, and 70% were branded in a foreign language (Tull, 2018).
Medicine Management Training: According to Celeste Sauls (2016), medicine management training is an important factor in improving stock management. Such training focusses on the principles and implications of using, selecting, distributing, and managing drugs effectively. Celeste discovered that only two participants were comfortable claiming that they had received medicine management training and were actively using it. Pharmacists are not the only ones who manage medicines; pharmacy assistants, nurses, and other healthcare staff must also be trained.
Medicines and supplies expire due to cold chain and logistical issues in healthcare institutions.According to Kraiselburd et al. (2013), access to vital medicines is contingent on well-established and operational supply chain networks. The cold-chain system should be able to transport pharmaceuticals from the manufacturer to the end user in healthcare institutions. Supply chain management in public sector health systems has garnered increased attention in recent years, serving as both a priority and a difficulty for many countries as governments strive to deliver a growing quantity of products.
According to a study conducted in Ethiopia by AWOL Jemal et al. (2019) on “Unused and Expired Medications,” the most common problem reported by all respondents was the Pharmaceuticals Fund and Supply Agency (PFSA) pushing program products and sometimes Revolving Drug Fund items that were near-expiry and/or not needed at health facilities. Other notable reasons reported by study participants included differing prescription patterns by prescribers, quantification issues (particularly for seasonal products), poor data quality, a poorly functioning Drug and Therapeutics Committee (DTC), a lack of data during service expansion, issues with reporting consumption data from wards, failure to consider quantity on order, and a lack of inventory management skill by the store manager.
The expiration of medicines poses a severe danger to developing countries’ already limited access to medicines. According to (Mwesigwa, 2006; MoH, 2006), vital drugs have expired at the National Medical Store in Entebbe and in some Ugandan district hospital shops. While a report published by WHO (2010) indicated that similar difficulties were also faced in countries such as Botswana, India, and the United Republic of Tanzania. The same study found that in five public outlets, four had disposed of (destroyed) medicines, two had exchanged medicines with their supplier, customers returned medicines in one outlet, and all had received medicines at reduced prices or as donations in the previous year, due to projected expiry. Expiration of drugs appears to be a general concern in all medical supply outlets.
Similarly, excessive inventory levels raise the risk of drugs expiring (Bukhari et al., 2010). This could be related to poor medicine quantification, which occurs when facilities acquire more drugs than they require. In South Sudan, a reproductive security status study done in 2014 by the United States Agency for International Development (USAID) discovered that some Primary Health Care Centres (PHCC) were overstocked and drugs were about to expire. As a result, having a large supply of drugs is not recommended because it may result in waste due to expiration in healthcare institutions.
In Indonesia, a 2014 investigation by Pharmacies Sans Frontières revealed that “extremely large quantities” of cough medicines and antibiotic tetracycline would expire before being utilised, causing more complications for authorities than benefiting the community. (Tull, 2018).
Pharmacy inventory management is a complex but crucial procedure in healthcare delivery systems. Health care facilities that do not have sufficient pharmacy inventory management processes risk failing to give patients with the most suitable medication when they are most in need. Addressing pharmacy inventory management and the revenue cycle efficiently can help organisations enhance financial performance, meet regulatory requirements, reduce patient safety risk, and maintain medication availability with fewer stock outs. Many health facilities and healthcare organisations use pharmacy organisation management systems to provide proper pharmaceutical responsibility and inventory traceability from procurement to patient administration or disposal. Effective and transparent tracking systems that enable pharmacies to precisely record inventory components such as pharmaceutical expiration dates and physical amounts may also help to prevent bad patient outcomes (Iqbal, Geer, & Dar, 2017).
Donated drugs that are distributed on a push basis lead to the expiration of medicines before they are provided to patients (Dias 2012). This occurs when facilities receive medications that they did not order. The donor’s belief is that because the health facilities do not have enough money to purchase drugs, they will accept whatever is offered. Medicines delivered in quantities greater than the normal consumption patterns will expire if not consumed entirely by the expiration date. Despite the Christian Medical Commission’s and WHO’s existing guidelines on rational medicine use, large amounts of expired or inappropriate medicines are found among donation stock from various donors, including humanitarian organisations, pharmaceutical industries, and governments (Tters, L,E, 2015).
The expiry date is the date on a product that the maker has determined beyond which the manufacturer will not guarantee the product’s potency, purity, or uniformity (Dias, 2012), and medicines will be regarded expired beyond this date. There is a shortage of medicines in public health facilities since the government relies heavily on donor cash to purchase medicines. These drugs are acquired and sent to facilities without their approval, resulting in cases where medicines expire in public health facilities simultaneously. Because drugs are expensive and pose a public health risk, there is a need to reduce their expiration in public health institutions in order to make the best use of limited resources.
Regulatory issues affecting the expiration of drugs and supplies in healthcare institutions
Nakyanziet al., (2019) in a study conducted in Uganda on Expiry of medicines in public health facilities and stores established that expiry of medicines in supply facilities was common among medicines for vertical health programs (with percentage of outlets reporting expiry), including vitamin A capsules, antiretroviral medicines, anti-tuberculosis agents, chloroquine, sulfadoxine/pyrimethamine, and nystatin tablets, though expiry of medicines such as anti-cancer agents,
It was also noticed that all of the top-expiring drugs are either essential (with a high consumption rate since they are utilised by the majority of the population) or critical (without them, the patient would die). Anticancer medications may expire due to delayed turnover due to their rarity and high cost. Similarly, tetracycline eye ointment and mebendazole have numerous better replacements, which may explain their poor turnover. According to Nakyanziet al. (2019), respondents’ perceptions of pharmaceutical expiration in retailers supported some of the study findings.
The poor management and coordination of a treatment policy change lead to the expiration of large stocks of chloroquine, sulfadoxine/pyrimethamine, and isoniazid in various Ugandan public health institutions (MoH, 2016). For example, effective cooperation among key parties can prevent expiration due to treatment policy changes and redundant procurement.
In 2010, a study of tracer drug supply in South Sudan revealed that 67% of health facilities employing the pull system lacked pharmaceutical management capacity in states and districts. Poor inventory management frequently results in a stockpile of expired medications (MOH, 2022).
In terms of medicine rotational policy, a system of medicine utilisation based on expiry date should be implemented to ensure appropriate stock rotation, such as FEFO. To avoid accidentally picking expired stock, keep it apart from usable stock. Expired medicines should be disposed of on a regular basis in accordance with disposal regulations in order to free up space and prevent expired medicines from being dispensed. Effective medication control in public service is required to maintain the high quality of pharmaceutical products (Perspectives W.H.O.P, 2004).
Theoretical Framework
The theoretical framework of this study was based on four theories: inventory control theory, supply chain management models, rational choice theory, and resource-based theory of competitive advantage, which are detailed below.
Inventory Control Theory and Supply Chain Management Models
Ford W. Harris devised the Inventory Control Theory, often known as the Economic Order Quantity (EOQ) model, in 1913, and R.H. improved it later on. Wilson in 1934 (Harris 1913; Wilson 1934). This theory focusses on establishing the ideal order quantity and inventory levels in supply chain management to reduce costs while increasing efficiency (Chopra & Meindl, 2010). The EOQ model assumes steady demand, a fixed lead time, and ordering expenses for each order placed. The EOQ model determines the optimal order quantity (Q) by weighing the costs of ordering (Co) and inventory storage (Ch) (Chopra & Meindl, 2010). This theory has found widespread application in a variety of domains, including logistics, operations management, and supply chain management (Jacobs & Chase, 2018). In the context of this study, the Inventory Control Theory can be used to interpret complaint handling as a supply chain process, with complaints representing the “demand” and the ERB’s reaction representing the “supply” (Bhandari 2008).
The Inventory Control Theory is relevant to this study because of its potential to improve complaint handling procedures (Kumar et al., 2017). Using the EOQ model, the research can establish the best response time and resource allocation to reduce complaint handling expenses. Furthermore, the theory can be utilised to discover areas for cost savings and efficiency improvements in the complaint handling process, resulting in improved service delivery and customer satisfaction (Santos, 2013). Overall, the Inventory Control Theory is a useful framework for analysing and optimising complaint handling procedures in supply chain management. On the other side, Supply Chain Management Models offer systematic techniques to controlling the flow of goods, information, and funds from suppliers to customers (Chopra & Meindl, 2010).
Rational choice of theories
This chapter discusses the theories that served as the foundation for the study’s theoretical and conceptual framework. A theoretical framework specifies the fundamental concept of research and identifies the relationships between them, so providing a structure for understanding and analysing a given phenomenon. (Sarah, 2023). It is a collection of interconnected concepts, theories, and ideas that guide the research process and assist explain the relationship between the variables being studied. The theoretical framework serves as a road map for research effort, providing a platform for reviewing current theories and forming arguments for use in study. As a result, in this study, resource-based theory will be applied to investigate the reasons associated with the high expiry rate of pharmaceutical items within the Ministry of Health’s supply chain: a case study of Choma District in Southern Province.
Supply Chain Management Theory
Supply Chain Management (SCM) Theory focusses on the effective integration and coordination of suppliers, manufacturers, warehouses, and retailers to guarantee that products are manufactured and supplied in the appropriate amounts, locations, and times. It includes all operations connected to the movement and transformation of goods from raw materials to end users, as well as the associated information flows. The notion of SCM has evolved throughout time, including notable contributions from researchers like as Martin Christopher (1992) and Donald J. Bowersox (2002).
SCM Theory is supported by studies by Chopra and Meindl (2016) and Simchi-Levi, Kaminsky, and Simchi-Levi (2008), which emphasise its importance in optimising logistics, lowering costs, and enhancing customer satisfaction. These studies emphasise the importance of supply chain management (SCM) in obtaining a competitive advantage through good integration and coordination. In this study, SCM Theory is used to better understand the logistical and cold-chain difficulties associated with medicinal items. It provides a framework for analysing the elements that contribute to pharmaceutical product expiration rates and developing strategies for improving supply chain management procedures to ensure medications are delivered on time and efficiently.
Behavioural Theory
Behavioural Theory seeks to comprehend and analyse human behaviour, specifically how individuals’ actions and decisions are influenced by their knowledge, attitudes, motives, and environmental circumstances. This hypothesis was developed by many psychologists, including B.F. Skinner (1953) emphasised the necessity of understanding behaviour through observable behaviours, as well as the environment’s influence on behaviour.
Fishbein and Ajzen (1975) and Bandura (1986) investigate how attitudes, beliefs, and perceptions influence behaviour, lending credence to Behavioural Theory. These studies shed light on how to predict and modify behaviour by understanding the underlying psychological elements (Fishbein and Ajzen, 1975; Bandura, 1986). This study uses behavioural theory to investigate health workers’ knowledge, attitudes, and practices around pharmaceutical management. It aids in identifying the behavioural aspects that contribute to the expiration of pharmaceutical items, as well as developing focused interventions to enhance health workers’ habits and prevent medication waste.
Conceptual framework
A conceptual framework is a research instrument that helps a researcher gain awareness and comprehension of the subject under investigation and express it. It is used in research to highlight potential paths of action or to propose a preferred approach to an idea or thought. Bogdan and Biklen (2003) define a conceptual Framework as a basic structure composed of abstract blocks that represent the observable, experiential, and analytical/synthetic aspects of a process or system under consideration. The integration of these pieces completes the foundation for specific intended results. The investigation of the independent variable and its influence on the independent variables allows for the discovery of answers to the research topic, which is represented by a model known as a conceptual framework (Sekaran, 2009). The independent variables in this study are health personnel’ qualities, cold chain and logistical factors, and regulatory factors, all of which have an impact on the dependent variable, which is the expiry of medicines and supplies at health facilities.
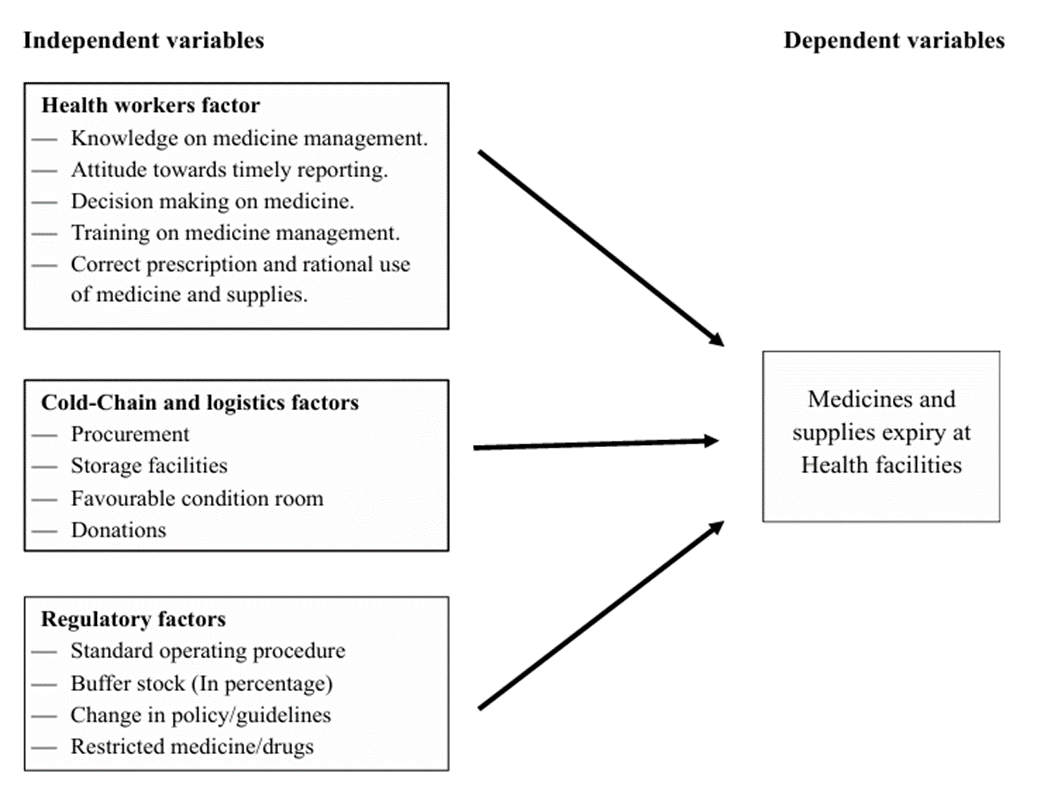
Figure 1: Shows factors associated with high expiry of medicines and supplies
METHODOLOGY
Research Philosophy
This study was founded on Pragmatism, as it used a mixed-method approach and a cross-sectional descriptive research design. Pragmatism combines quantitative and qualitative methodologies to successfully address real-world problems, emphasising practical solutions above strict theoretical perspectives (Tashakkori & Teddlie, 2010). This approach enabled the study to investigate the high expiry rate of pharmaceutical items, integrating subjective insights from healthcare professionals with statistical data analysis to provide a comprehensive picture of medicine waste.
Research Design
The study took a mixed-methods approach using a cross-sectional descriptive research design. The mixed-method approach combines qualitative (interviews, observations) and quantitative (survey, inventory analysis) approaches to provide a thorough assessment of health worker-related factors, cold-chain logistics, and regulatory frameworks that influence medicine expiry. The cross-sectional design allowed for data gathering from various health facilities at one time, resulting in a more comprehensive research approach. This study used a combination of deductive and inductive methodologies. Deductive analysis was utilised to examine existing theories such as Inventory Control Theory, Rational Choice Theory, and Resource-Based Theory, whilst inductive reasoning allowed for pattern recognition and hypothesis formation using the obtained data (Tracy, 2019).
Research Onion
The study’s approach was structured using the Research Onion Model developed by Saunders, Lewis, and Thornhill (2016). This systematic framework promotes structured decision-making across study philosophy, approach, strategy, and data gathering methodologies. The updated Research Onion model gave direction in selecting practical approaches for analysing pharmaceutical expiry trends in Choma District health facilities.

Figure 2: Research questions
Research Choice
This study used a mixed-methods approach, combining qualitative and quantitative data analysis to determine the factors that contribute to medicine expiration, the level of inventory inefficiencies, and the impact of storage and logistics infrastructure. Numerical data (expiry rates, facility storage state) and descriptive insights (health worker perceptions, regulatory enforcement gaps) were analysed together, resulting in more complete findings (Creswell, 2014).
Population of the Study
Healthcare personnel in Choma District, Southern Province, who work in pharmaceutical supply chain management, such as dispensing, storage, inventory tracking, and procurement, were the intended target population. The study included employees from various public health facilities, such as chemists, nurses, medical officers, supply-chain managers, dispensers, and cold-chain supervisors. Choma District was chosen owing to its strong demand for pharmaceutical products and continuous issues with medication expiration management. A total of 35 people were polled and interviewed to gain views from professionals who are actively managing drug inventory.
Sampling and Sample Size
A stratified random sample technique was used to guarantee a broad representation across health institution types. The population of health facilities was separated into several strata depending on facility size, kind, and location, with a random sample drawn from each. This strategy reduced selection bias and increased the generalisability of findings. A sample size of 35 participants was chosen, comprising PHCC administrators, chemists, supply-chain officers, and clinical officers, to ensure diverse perspectives on pharmaceutical management.
Data Collection Methods
Data was collected using both quantitative (structured surveys, numerical inventory analysis) and qualitative (interviews, focus groups, document reviews) approaches. Surveys gathered numerical data on pharmaceutical expiry rates, storage adequacy, and purchase habits, while interviews elicited expert viewpoints, regulatory hurdles, and facility-specific issues.
Pilot Study
A pilot study was undertaken at Choma District’s public health institutions to test and enhance data collection devices, guaranteeing clarity and effectiveness prior to the full-scale study. The survey questions and interview techniques were modified to improve validity and reliability.
Data analysis
This study employed a concurrent triangulation technique, combining quantitative and qualitative data analysis, to thoroughly investigate factors influencing pharmaceutical expiry in healthcare institutions. Quantitative examination of numerical survey responses and inventory records revealed trends and patterns in medicine expiry rates, highlighting high-risk categories such as donated drugs and vital pharmaceuticals. Qualitative analysis of interview transcripts and observational notes yielded themes on health worker behaviours, supply chain inefficiencies, regulatory gaps, and logistical issues, which were then cross-referenced with quantitative patterns to guarantee consistency and dependability. The triangulation of findings from both data sources improved validity, offered a more comprehensive knowledge, and resulted in well-supported conclusions and practical suggestions.
Ethical considerations
This study received authorisation and clearance from the University of Zambia Graduate School of Business, the University Ethics Committee, the Provincial Health Office, the District Health Office, and health facilities. Participants provided informed consent prior to data collection, and confidentiality was ensured by keeping all data under lock and key and using it solely for the purposes of this study.
RESULTS PRESENTATION
Demographic Information
The study included a diverse group of healthcare workers with varying demographic characteristics: ages ranged from 25 to 55 years (32% aged 25-34, 40% aged 35-44, and 28% aged 45-55); 56% were male and 44% female; 48% held a diploma and 52% a degree; 44% were single and 56% married; and years of experience varied, with 36% having 5-10 years, 40% having 11-20 years, and 24% having 21-30 years in healthcare.
Table 1: Demographic Information
| Demographic Variable | Category | Number of Participants | Percentage (%) |
| Age | 25 – 34 years | 8 | 32 |
| 35 – 44 years | 10 | 40 | |
| 45 – 55 years | 7 | 28 | |
| Gender | Male | 14 | 56 |
| Female | 11 | 44 | |
| Education Level | Diploma | 12 | 48 |
| Degree | 13 | 52 | |
| Marital Status | Single | 11 | 44 |
| Married | 14 | 56 | |
| Years of Experience in Healthcare Service | 5 – 10 years | 9 | 36 |
| 11 – 20 years | 10 | 40 | |
| 21 – 30 years | 6 | 24 |
Source: Primary data collection: 2024
Expiry of Medicines and Supplies: Proportion of Available Medicines and Supplies with High Expiry in Health Facilities
Data acquired from health facilities in Choma District, Southern Province, show trends in pharmaceutical stock expiration. The data show that a large number of medicines and supplies had expired, implying inefficiencies in inventory management, procurement planning, and supply chain coordination. 78.3% of all drugs in stock were expired, indicating significant gaps in predicted demand and stock rotation policies. Essential pharmaceuticals, which are critical for healthcare service delivery, have a 56.5% expiry rate, raising concerns regarding procurement and storage practices. Family planning items had a lower expiry rate of 8.7%, which could imply improved inventory management or increased demand stability. However, the expiry rate for donated pharmaceuticals was shockingly high at 65.2%, indicating problems with delivery delays and storage limits. The high rate of outdated medicines and supplies has serious consequences for healthcare service delivery. Expired vital drugs can cause treatment disruptions, erode patient trust, and raise expenses due to waste. Inefficient administration of donated drugs, in particular, emphasises the need for better cooperation between donors and healthcare facilities to ensure timely distribution and utilisation. Strengthening inventory tracking systems, optimising procurement tactics, and implementing improved stock management techniques can all help to reduce these issues, minimising pharmaceutical waste and increasing overall service delivery in healthcare facilities.
Table 2: Proportion of Available Medicines and Supplies with High Expiry in Health Facilities
| Variables | Categories | Frequency (N=23) | Percentage (%) |
| All Medicines in Stock | Expire (Yes) | 18 | 78.3 |
| Expire (No) | 5 | 21.7 | |
| Essential Medicines | Expire (Yes) | 13 | 56.5 |
| Expire (No) | 10 | 43.5 | |
| Family Planning Products | Expire (Yes) | 2 | 8.7 |
| Expire (No) | 21 | 91.3 | |
| Donated Medicine | Expire (Yes) | 15 | 65.2 |
| Expire (No) | 8 | 34.8 |
Source: Primary data collection: 2024
Participant 3:
“Yes, we do experience expiries, especially with antibiotics and vaccines. They tend to pile up and eventually go past their expiration dates. This is often due to a combination of factors, including overstocking, inadequate storage facilities, and insufficient demand. As a result, these lifesaving medications are rendered unusable, which can have serious consequences for patients in need. It’s a complex issue that requires careful inventory management, coordination with suppliers, and strategic planning to minimize waste and ensure that patients receive the medications they need.”
Participant 5:
“Antiretrovirals and painkillers often expire because we receive more than we can dispense within the shelf life. This can happen when there’s a surge in donations or shipments, and our storage facilities are not equipped to handle the excess. Additionally, the high volume of medications can lead to errors in inventory management, causing some items to be overlooked or misplaced. To mitigate this issue, we’re working to improve our inventory management systems, enhance our storage facilities, and establish stronger relationships with our suppliers to better anticipate and manage our medication needs.”
Univariate Analysis of Health Worker and System-Level Factors Associated with Medicine Expiry
This table provides a standalone overview of frequencies and proportions for each variable measured in the study without comparing expired vs. non-expired outcomes. It offers insight into the overall distribution of demographic, professional, and logistical characteristics of the surveyed health workers and facilities. The study involved 23 healthcare workers, the majority (73.9%) of whom had over two years of experience at their current facility. Despite this, extensive expiry of pharmaceutical products was reported, prompting deeper investigation into systemic drivers. In terms of knowledge, 82.6% of respondents rated their skills as either “very good” (47.8%) or “excellent” (34.8%), yet this did not correlate with lower medicine expiry rates. Regarding attitude toward inventory reporting, 56.5% rated theirs as “good” while 30.4% described it as “fairly good,” indicating variability in vigilance. Most participants (82.6%) were actively involved in medicine and supply decision-making, yet this did not appear to reduce expiry rates—suggesting that involvement alone may not be sufficient without effective systems. Concerning logistical factors, 56.5% of facilities received near-expiry donor medicines, and 65.2% cited weak coordination with donor agencies. Importantly, only 17.4% of facilities used real-time inventory tracking systems, a critical gap considering its relevance for expiry forecasting and automated alerts.
Table 3: Univariate Analysis of Health Worker and System-Level Factors Associated with Medicine Expiry
| Variable | Category | Frequency (N=23) | Percentage (%) |
| Working Period | > 2 Years | 17 | 73.9 |
| < 2 Years Combined | 6 | 26.1 | |
| Level of Knowledge | Very Good + Excellent | 19 | 82.6 |
| Fair + Good | 4 | 17.4 | |
| Health Worker Attitude | Good | 13 | 56.5 |
| Fairly Good | 7 | 30.4 | |
| Other | 3 | 13.0 | |
| Participating in Decision Making | Yes | 19 | 82.6 |
| No | 4 | 17.4 | |
| Medicine Use Rationale | Every Patient | 16 | 69.6 |
| Clinical Need | 5 | 21.7 | |
| Other or Missing | 2 | 8.7 | |
| Donor Shelf Life Quality | Near-Expiry | 13 | 56.5 |
| Adequate Shelf Life | 10 | 43.5 | |
| Donor Coordination Strength | Weak | 15 | 65.2 |
| Strong | 8 | 34.8 | |
| Real-Time Inventory System Use | No | 19 | 82.6 |
| Yes | 4 | 17.4 |
Bivariate Analysis of Factors Associated with High Medicine Expiry
This table uses chi-square analysis to determine whether particular variables have statistically significant relationships with drug expiry outcomes. It compares categorical replies from establishments reporting expired and non-expired medications. The bivariate study intended to see if specific health professional qualities and systemic factors were statistically connected with high medication expiration rates. While none of the factors were statistically significant (p > 0.05), a few noteworthy tendencies appeared. The level of knowledge produced a chi-square (χ²) value of 2.361 and a p-value of 0.501. 50% of those evaluating their knowledge as “very good” reported expired stock, compared to 27.8% of “excellent” respondents, indicating that training quality may require greater inspection. Health workers’ attitudes towards inventory reporting showed a χ² of 3.784 and p = 0.286, revealing that 38.9% with “fairly good” attitudes and 50% with “good” attitudes still suffered expiries, indicating that personal viewpoint had modest influence on stock outcomes. Participation in medical management choices had a χ² of 0.030 and p = 0.862. There was no significant difference between those participating (83.3%) and uninvolved (16.7%), indicating structural or communication difficulties. Donor shelf life quality generated χ² = 2.788 and p = 0.426. 61.1% of institutions receiving near-expiry stock reported wastage, compared to 38.9% receiving medications with appropriate life, indicating donor policy gaps. Donor coordination strength was equally telling (χ² = 3.345, p = 0.341), with 72.2% of weakly coordinated sites reporting expiries compared to 27.8% with good coordination. The usage of real-time inventory systems resulted in the greatest differential (χ² = 4.711, p = 0.245), with 88.9% of facilities missing these systems experiencing expiries compared to just 11.1% of those utilising them. This highlights the importance of digital solutions in reducing loss. Although these connections were not statistically significant, the emerging trends reveal key operational inefficiencies particularly in donor management, technical infrastructure, and supply chain oversight that necessitate system-wide improvements in accordance with WHO regulations.
Table 4: Bivariate Analysis of Factors Associated with High Medicine Expiry
| Variable | Category | Expired (Yes) | Expired (No) | Total (N=23) | I | P-value |
| Level of Knowledge | Higher (VG + Exc) | 14 (77.8%) | 5 (100.0%) | 19 | 2.361 | 0.501 |
| Lower (Fair + Good) | 4 (22.2%) | 0 (0.0%) | 4 | |||
| Health Worker Attitude | Good | 9 (50.0%) | 4 (80.0%) | 13 | 3.784 | 0.286 |
| Fairly Good or Other | 9 (50.0%) | 1 (20.0%) | 10 | |||
| Decision Making Participation | Yes | 15 (83.3%) | 4 (80.0%) | 19 | 0.030 | 0.862 |
| No | 3 (16.7%) | 1 (20.0%) | 4 | |||
| Use Rationale | Every Patient | 16 (88.9%) | 4 (80.0%) | 20 | 0.664 | 0.882 |
| Clinical Need + Other | 3 (11.1%) | 1 (20.0%) | 3 | |||
| Donor Shelf-Life Quality | Near-Expiry | 11 (61.1%) | 2 (40.0%) | 13 | 2.788 | 0.426 |
| Adequate Shelf Life | 7 (38.9%) | 3 (60.0%) | 10 | |||
| Donor Coordination Strength | Weak | 13 (72.2%) | 2 (40.0%) | 15 | 3.345 | 0.341 |
| Strong | 5 (27.8%) | 3 (60.0%) | 8 | |||
| Real-Time Inventory System Use | No | 16 (88.9%) | 3 (60.0%) | 19 | 4.711 | 0.245 |
| Yes | 2 (11.1%) | 2 (40.0%) | 4 |
Qualitative responses
Participants in Choma District identified several health worker-related factors contributing to the expiry of medicines and supplies. Insufficient knowledge regarding proper storage and management practices was a common theme, indicating a need for better training and education. Additionally, a lack of motivation and responsibility among health workers towards managing inventories effectively was noted. Participants also highlighted instances of irrational prescribing and dispensing practices, which contribute to medicines expiring before they are used.
Participant 3:
“Many of our staff are not well-trained in inventory management, which leads to poor handling and storage of medicines. This is a critical issue, as improper storage can compromise the efficacy and safety of the medications. Furthermore, inadequate training can result in inaccurate inventory tracking, leading to stockouts or overstocking. To address this, we need to invest in comprehensive training programs for our staff, focusing on best practices in inventory management, pharmacological knowledge, and quality control measures.”
Participant 7:
“There seems to be a lack of motivation among some health workers to take responsibility for managing inventories properly. This can be attributed to various factors, including inadequate resources, insufficient supervision, and a lack of accountability. When health workers are not motivated to manage inventories effectively, it can lead to a range of problems, including medication shortages, expired or damaged products, and inefficient use of resources. To overcome this challenge, we need to foster a culture of accountability, provide incentives for good performance, and ensure that health workers have the necessary resources and support to excel in their roles.”
Participant 2:
“I have seen instances where medicines are prescribed or dispensed irrationally, leading to unnecessary wastage. This can occur due to a lack of adherence to clinical guidelines, inadequate patient education, or insufficient monitoring of medication use. Irrational prescribing and dispensing practices not only waste valuable resources but also pose serious health risks to patients. To address this issue, we need to implement evidence-based prescribing guidelines, enhance patient education and counseling, and establish robust monitoring and evaluation systems to track medication use and outcomes.”
Cold-chain and logistic factors associated with medicines & supplies expiry at health facilities.
The findings from Choma District reveal key cold-chain and logistical challenges contributing to the expiry of medicines and supplies. 91.3% of respondents reported having adequate storage facilities, while 8.7% indicated inadequate storage, resorting to alternative solutions such as keeping medicines in offices, which could compromise temperature control and overall drug efficacy. Regarding storage facility standards, 60.9% of respondents rated their storage conditions as acceptable, while 39.1% considered them unacceptable, suggesting inconsistencies in storage management practices. 82.6% reported experiencing medicine and supply expiry, demonstrating widespread inefficiencies in stock rotation and monitoring. Among those reporting expiries, occurrences varied, with 34.8% experiencing them every three months, 30.4% monthly, 13.0% every six months, and a smaller proportion (4.3%) facing weekly expiries, highlighting differences in facility inventory control mechanisms. Major contributing factors included poor storage practices (34.8%), lack of qualified personnel (13.0%), and overstocking (65.2%), suggesting procurement inefficiencies and excess supply beyond patient consumption rates. Additionally, 34.8% of respondents admitted to not knowing the actual number of patients accessing the facility, indicating gaps in demand forecasting that could lead to excessive stock levels and increased expiry risks. 87.0% reported that partners procure medicines, which may affect local supply chain coordination. To mitigate these challenges, improved storage infrastructure, better regulatory oversight, enhanced forecasting techniques, and optimized procurement strategies are required to reduce medicine wastage and ensure supply chain efficiency.
Table 5: Univariate Analysis of Cold-Chain and Logistic Factors Associated with High Expiry of Medicines and Supplies
| Variables | Categories | Frequency (N=23) | Percentage (%) |
| Adequate Storage Facility | Yes | 21 | 91.3 |
| No | 2 | 8.7 | |
| Alternative Storage Facilities | Office Storage | 2 | 8.7 |
| Not Applicable | 21 | 91.3 | |
| Opinion of Storage Standards | Acceptable | 14 | 60.9 |
| Unacceptable | 9 | 39.1 | |
| Experience Medicines and Supplies Expiry | Yes | 19 | 82.6 |
| No | 4 | 17.4 | |
| Frequency of Expiry Occurrence | Weekly | 1 | 4.3 |
| Monthly | 7 | 30.4 | |
| Every 3 Months | 8 | 34.8 | |
| Every 6 Months | 3 | 13 | |
| Missing Data | 4 | 17.4 | |
| Poor Storage Facility | Yes | 8 | 34.8 |
| No | 15 | 65.2 | |
| Lack of Qualified Personnel | Yes | 3 | 13 |
| No | 20 | 87 | |
| Overstocking of Medicines and Supplies | Yes | 15 | 65.2 |
| No | 8 | 34.8 | |
| Unknown Patient Demand | Yes | 8 | 34.8 |
| No | 15 | 65.2 | |
| Partners Procure Medicines | Yes | 3 | 13 |
| No | 20 | 87 |
Source: Primary data collection: 2024
Table 6: Bivariate Analysis of Cold-Chain and Logistic Factors Associated with High Expiry of Medicines and Supplies
| Variables | Categories | Have Expired Medicines (Yes) | Have Expired Medicines (No) | Total (N=23) | Chi-Square (χ²) | P-value |
| Adequate Storage Facility | Yes | 16 (88.9%) | 5 (100.0%) | 21 (91.3%) | 0.608 | 0.435 |
| No | 2 (11.1%) | 0 (0.0%) | 2 (8.7%) | |||
| Alternative Storage Facilities | Office Storage | 2 (11.1%) | 0 (0.0%) | 2 (8.7%) | 0.608 | 0.435 |
| Not Applicable | 16 (88.9%) | 5 (100.0%) | 21 (91.3%) | |||
| Opinion of Storage Standards | Acceptable | 10 (55.6%) | 4 (80.0%) | 14 (60.9%) | 0.982 | 0.322 |
| Unacceptable | 8 (44.4%) | 1 (20.0%) | 9 (39.1%) | |||
| Experience Medicines and Supplies Expiry | Yes | 16 (88.9%) | 3 (60.0%) | 19 (82.6%) | 2.273 | 0.194 |
| No | 2 (11.1%) | 2 (40.0%) | 4 (17.4%) | |||
| Frequency of Expiry Occurrence | Weekly | 1 (5.6%) | 0 (0.0%) | 1 (4.3%) | 8.061 | 0.089 |
| Monthly | 7 (38.9%) | 0 (0.0%) | 7 (30.4%) | |||
| Every 3 Months | 7 (38.9%) | 1 (20.0%) | 8 (34.8%) | |||
| Every 6 Months | 1 (5.6%) | 2 (40.0%) | 3 (13.0%) | |||
| Poor Storage Facility | Yes | 7 (38.9%) | 1 (20.0%) | 8 (34.8%) | 0.615 | 0.621 |
| No | 11 (61.1%) | 4 (80.0%) | 15 (65.2%) | |||
| Overstocking of Medicines and Supplies | Yes | 14 (77.8%) | 1 (20.0%) | 15 (65.2%) | 5.759 | 0.033* |
| No | 4 (22.2%) | 4 (80.0%) | 8 (34.8%) | |||
Source: Primary data collection: 2024
The results indicate no statistically significant association between cold-chain and logistic factors and medicine expiry, except for overstocking (p<0.033). Overstocking combined with low patient consumption rates increases the likelihood of medicines reaching their expiration date before being used. Strengthening inventory control and refining forecasting mechanisms could help mitigate this issue and optimize stock utilization.
Participant’s Responses
Participant 8:
Our refrigeration units often malfunction, causing temperature fluctuations that degrade medicines. This is a major concern for us, as even slight deviations from the recommended temperature range can render vaccines and medications ineffective. When our refrigeration units fail, we’re forced to rely on backup systems, which may not always be available or reliable. This can lead to a loss of valuable medications and vaccines, ultimately affecting the health and well-being of our patients.”
Participant 11:
“Power outages are a big problem. Without reliable backup, our vaccines and other sensitive medicines suffer. We’ve experienced instances where power outages have lasted for hours, causing our refrigeration units to fail and putting our entire stock of vaccines and medications at risk. This not only wastes valuable resources but also compromises the health and safety of our patients. We urgently need a reliable backup power system to ensure that our cold chain remains uninterrupted.”
Participant 13:
“We do not have enough monitoring equipment to ensure that our cold-chain conditions are consistently maintained. This lack of visibility makes it difficult for us to identify potential issues before they become major problems. Without real-time monitoring, we’re forced to rely on manual checks, which can be time-consuming and prone to human error. Investing in modern monitoring equipment would enable us to maintain optimal cold-chain conditions, reduce the risk of medication degradation, and provide better care for our patients…our refrigeration units often malfunction, causing temperature fluctuations that degrade the medicines.”
Regulatory considerations affecting medicine and supply expiration in health facilities in Choma District.
The results in this study revealed important regulatory elements influencing pharmaceutical and supply expiry dates. According to the statistics, 87.0% of respondents acknowledged the presence of standard operating procedures (SOPs) in their facilities, with 13.0% reporting the absence of SOPs. The absence of SOPs in some facilities may contribute to inefficiencies in inventory management, resulting in higher expiry rates. Furthermore, 87.0% of respondents claimed that no regular checks were performed, while only 13.0% acknowledged that their facilities performed routine monitoring. Inadequate checks can lead to stock mismanagement and a failure to notice and handle potential expiry concerns in a timely manner. Understanding the disease burden has also surfaced as a regulatory concern, with 91.3% reporting a lack of awareness of the disease burden, implying that medicines may not be ordered in accordance with demand. Furthermore, 91.3% of respondents reported that medicine orders were not in line with facility consumption trends, indicating a gap between procurement plans and real-time usage requirements. Another big difficulty was accurate medicine demand estimation, with 91.3% saying that their facilities lacked effective forecasting procedures, raising the risk of overstocking and expiry. To address these issues, 78.3% of respondents said they added buffer stock mostly to minimise stock-outs, while others cited unexpected lead times and logistical constraints such long distances to suppliers. In cases where drugs expired, 69.6% stated that the expiry dates were too near at the time of delivery, resulting in fast deterioration before use. 13.0% stated that a lack of appropriate patients contributed to expiry, while 8.7% ascribed it to a lack of physicians to provide the medications. Strengthening forecasting models, increasing regulatory supervision, and ensuring timely stock rotation could all assist to solve inefficiencies and decrease waste in drug supply chains.
Table 7: Univariate Analysis of Regulatory Factors Associated with High Expiry of Medicines and Supplies
| Variables | Categories | Frequency (N=23) | Percentage (%) |
| Standard Operating Procedure | Yes | 20 | 87 |
| No | 3 | 13 | |
| Regular Checks | Yes | 3 | 13 |
| No | 20 | 87 | |
| Understand Disease Burden | Yes | 2 | 8.7 |
| No | 21 | 91.3 | |
| Ordering Based on Consumption | Yes | 2 | 8.7 |
| No | 21 | 91.3 | |
| Accurate Projection | Yes | 2 | 8.7 |
| No | 21 | 91.3 | |
| Reason for Adding Buffer Stock | To Avoid Stock-outs | 18 | 78.3 |
| Unpredictable Lead Time | 3 | 13 | |
| Long-distance Challenges | 2 | 8.7 | |
| Received Restricted Medicines | Yes | 3 | 13 |
| No | 20 | 87 | |
| Cases Where Medicines Expired | Yes | 2 | 8.7 |
| No | 21 | 91.3 |
Source: Primary data collection: 2024
Table 8: Bivariate Analysis of Regulatory Factors Associated with High Expiry of Medicines and Supplies
| Variables | Categories | Have Expired Medicines (Yes) | Have Expired Medicines (No) | Total (N=23) | Chi-Square (χ²) | P-value |
| Standard Operating Procedure | Yes | 15 (83.3%) | 5 (100.0%) | 20 (87.0%) | 0.958 | 1 |
| No | 3 (16.7%) | 0 (0.0%) | 3 (13.0%) | |||
| Regular Checks | Yes | 3 (16.7%) | 0 (0.0%) | 3 (13.0%) | 0.958 | 1 |
| No | 15 (83.3%) | 5 (100.0%) | 20 (87.0%) | |||
| Understand Disease Burden | Yes | 2 (11.1%) | 0 (0.0%) | 2 (8.7%) | 0.608 | 1 |
| No | 16 (88.9%) | 5 (100.0%) | 21 (91.3%) | |||
| Ordering Based on Facility Consumption | Yes | 2 (11.1%) | 0 (0.0%) | 2 (8.7%) | 0.608 | 1 |
| No | 16 (88.9%) | 5 (100.0%) | 21 (91.3%) | |||
| Accurate Projection | Yes | 2 (11.1%) | 0 (0.0%) | 2 (8.7%) | 0.608 | 1 |
| No | 16 (88.9%) | 5 (100.0%) | 21 (91.3%) | |||
Source: Primary data collection: 2024
These results indicate no statistically significant relationship between regulatory factors and the expiry of medicines and supplies in this study. However, the data highlights gaps in stock monitoring, disease burden awareness, and procurement planning, emphasizing the need for strengthened regulatory oversight and strategic inventory management in healthcare facilities.
Participant’s responses
Participant 23:
“We face frequent delays in deliveries, resulting in medicines arriving with very little shelf life left. This is particularly concerning for temperature-sensitive medications, which require precise storage conditions to maintain their potency. When deliveries are delayed, these medications are at risk of degradation, which can render them ineffective or even unsafe for patient use. To mitigate this issue, we’re exploring alternative shipping methods and partnering with suppliers who can provide more reliable and expedited delivery options.”
Participant 11:
“Overstocking is a common issue. We receive large quantities without accurate demand forecasting, leading to wastage. This not only results in significant financial losses but also contributes to the already pressing problem of medication waste. To address this challenge, we’re working to implement a more sophisticated inventory management system that takes into account real-time demand data and allows for more precise forecasting. By doing so, we hope to reduce waste, optimize our inventory, and ultimately improve our ability to provide patients with the medications they need.”
Participant 9
“Our inventory management system is outdated and ineffective, making it difficult to track and rotate stock efficiently. This leads to a range of problems, including stockouts, overstocking, and medication waste. To address this issue, we’re investing in a modern, cloud-based inventory management system that will enable us to track our inventory in real-time, receive automated alerts when medications are approaching expiration, and optimize our storage and rotation procedures. By upgrading our inventory management system, we aim to improve our operational efficiency, reduce waste, and enhance our ability to provide high-quality patient care.”
Participant 15:
“There is a clear lack of enforcement when it comes to inventory management regulations. This leads to many avoidable expiries. In many cases, healthcare facilities and pharmacies are not held accountable for their inventory management practices, which can result in a lack of attention to detail and a higher risk of expiries. Furthermore, the absence of standardization in inventory management practices across different facilities and regions exacerbates the problem. To address this issue, we need stricter enforcement of regulations, regular audits, and training programs to ensure that healthcare professionals are equipped to manage inventory effectively.”
Participant 6:
“Our policies are not robust enough. Even where policies exist, they are often not implemented properly, causing inefficiencies. This is a systemic issue that affects not only inventory management but also the overall quality of care. Weak policies and inadequate implementation lead to a lack of standardization, poor communication, and insufficient training. As a result, healthcare professionals are often left to navigate complex inventory management systems without the necessary guidance or support. To address this issue, we need to develop and implement more comprehensive policies, provide regular training and support, and ensure that policies are consistently enforced across all facilities and regions.
DISCUSSION
This study identified major issues in pharmaceutical supply chain management, notably those related to the expiration of key drugs such as antibiotics, antiretrovirals, vaccinations, and painkillers, which are consistent with global findings (Management Sciences for Health 2012). With 78.3% of health facilities reporting expired supplies, the data suggests systematic inefficiencies rather than individual mismanagement. Prior study (Su & Knechel, 2019; Nakyanziet et al., 2009) supports this narrative by correlating frequent drug waste to inadequate inventory techniques and storage limits. In support of Inventory Control Theory, which emphasises demand-driven procurement and timely stock rotation, the study found that continual delivery of near-expiry pharmaceuticals was a substantial contributor to waste, particularly among donated supplies (65.2% expiry rate). The Resource-Based Theory explains how donations, which are frequently disconnected from treatment regimens, result in redundant stock accumulation and loss (Kraiselburd et al., 2013).
Despite 73.9% of respondents having more than two years of experience and 82.6% participating in medication management decisions, bivariate analysis revealed no statistically significant relationship between these parameters and medicine expiry (χ² = 0.030, p = 0.862). This shows that practical decision-making frameworks and organisational mechanisms may outperform personal expertise in reducing waste. Despite 82.6% rating their knowledge as “very good” or “excellent,” expiration remained high, with no significant correlation identified (χ² = 2.361, p = 0.501), indicating that simple awareness is insufficient without applied training and supportive infrastructure.
Attitudes towards timely reporting were not statistically significant (χ² = 3.784, p = 0.286), however 50% of participants who assessed their attitude as “good” nevertheless reported expired stock, revealing operational inadequacies. Similarly, justification for medicine use showed no relevant correlation (χ² = 0.664, p = 0.882). 69.6% giving medicines to every patient rather than based on clinical need, indicating poor demand assessment.
System-level inefficiencies were more apparent. Facilities receiving near-expiry gifts were more likely to report expiries (61.1%) compared to those getting properly dated stock (38.9%), but this was not statistically significant (χ² = 2.788, p = 0.426). Weak donor coordination was associated with a 72.2% expiry rate, while strongly coordinated sites had a 27.8% rate (χ² = 3.345, p = 0.341). This suggests a logistical imbalance between donor organisations and health authorities. Facilities without real-time inventory tracking systems had significantly higher expiry rates (88.9%) compared to those with such systems (11.1%) (χ² = 4.711, p = 0.245). This highlights the importance of digital infrastructure in reducing expiry, aligning with both Inventory Control and Resource-Based Theories.
Storage conditions exacerbated supply chain management challenges. While 91.3% of respondents reported appropriate storage, qualitative insights highlighted a dependency on office premises and poor cold-chain compliance, with 39.1% citing inadequate infrastructure. Sauls (2016) and the Ministry of Health Malaysia (2011) highlight how storage misalignment and a lack of environmental controls might expedite pharmaceutical spoilage. Despite SOP presence at 87.0% of sites and buffer stock policies in 78.3%, regulatory enforcement was variable. Prior reviews in Uganda and South Sudan identified inadequate policy implementation as a cause of drug expiry (Building Pharmaceutical Management Capacity, 2017; Uganda MOH, 2006).
Theoretical models, such as Rational Choice Theory, explain how information gaps, policy inertia, and logistical obstacles interact to reduce stock longevity. Essential improvements include strengthening regulatory audits, implementing forecast-based procurement, integrating real-time inventory systems, and formalising donor coordination protocols. Though statistical connections were not significant, data trends highlight systemic weaknesses that, if not addressed, will continue to jeopardise drug availability and public health outcomes.
CONCLUSION
The study reveals that drug expiration in Choma District health institutions is caused by systemic inefficiencies in inventory control, donor coordination, cold-chain logistics, and procurement planning. Although the majority of healthcare personnel were experienced and participated in medicine management, individual characteristics such as knowledge and decision-making participation could not clearly prevent expiry, implying that structural and operational factors are more important. Notably, several facilities received donor medicines that were about to expire and lacked adequate coordination with contributing agencies, resulting in hoarding and wastage. The lack of digital inventory systems exacerbated these issues, preventing effective stock rotation and expiry forecasts. Despite widespread assertions of adequate storage, observational data indicated anomalies, with pharmaceuticals frequently stored in unsuitable office settings, indicating gaps in cold-chain infrastructure and compliance. Finally, the findings highlight the need for system-wide reforms in procurement, inventory monitoring, storage standards, and regulatory control. Medicine waste is the outcome of linked logistical, infrastructural, and policy flaws. enhancing digital tools, fine-tuning donation policies, and increasing enforcement of standard operating procedures will be crucial to enhancing pharmaceutical management and healthcare outcomes.
RECOMMENDATIONS
Based on study findings and observed patterns, the following strategies are recommended to address medicine expiry in health facilities:
- Implement real-time stock tracking systems and demand-based forecasting models to reduce overstocking and ensure timely stock rotation.
- Provide continuous training on medicine handling, storage techniques, and pharmaceutical inventory planning to elevate practical expertise.
- Address facility storage gaps, enforce WHO cold-chain guidelines, and optimize medicine distribution networks to preserve drug efficacy.
- Establish donor protocols requiring minimum shelf-life guarantees, advance coordination on demand needs, and centralized donation tracking.
- Strengthen SOP compliance audits, adopt adaptable procurement models, and enforce performance indicators including expiry tracking metrics.
Author Contributions: Conceptualization, methodology writing review and editing and analysis (Bupe Bwalya) The author has decided to publish this version of the review article, Editing the article (Prof. Bupe Getrude Mutono-Mwanza)
Funding: Funding for this research was not provided. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Institutional Review Board Statement: This study was approved by the University of Zambia Humanities and Social Sciences Ethics Committee.
Informed Consent Statement: Not applicable.
Data Availability Statement: The datasets used during the current study are available from the corresponding author on rational request.
Acknowledgements: Firstly, I would like to give all the glory to God for making it possible for me to undertake my studies. Secondly, to my Lovely Wife, Jane Mutale Ngandwe, My Son, Twange Emmanuel Bwalya and my sisters for their unwavering love and support throughout the course of my studies. Thirdly, I would like to appreciate the effort made by the supervisor – Prof. Bupe Getrude Mutono-Mwanza in motivating, encouraging and showing me that the study is of supreme importance and leading me towards a point of success.
Finally, I would like to acknowledge the effort made by all participants with their valuable views which made this study a success. I thank the Provincial Health Office, Choma District Health Office and Facility Staff for giving me access to the facilities for data collection. God Bless you all.
Conflicts of Interest: The authors declare no conflict of interest.
REFERENCES
- Alex, L.E. (2018) ‘Factors Associated With the High Expiry Rate of Medecines and Supplies in Public Health Facilities in Jubek State , South Sudan’, EAC Regional Centres of Excellence for Vaccines, immunization and health supply chain management [Preprint].
- Aghalaya, S., Elias, A., & Pati, K. (2012). Analysing Reverse Logistics in the Indian Pharmaceuticals Industry: A Systems Approach. Mombai.
- Alnahas F, Yeboah P, Fliedel L, Abdin AY, Alhareth K. Expired medication: Societal, regulatory and ethical aspects of a wasted opportunity. Int. J. Environ. Res. Public Health. 2020; 17(3):787. 2.
- Bank, W. (2008). Enhancing public supply chain management in Zambia.
- Bero, L., Carson, B., Moller, H., & Hill, a. (2010). Compliance with WHO guidelines for drug donations during 2000–2008. Bulletin of the World Health Organization, Issue 88, pp. 922–929.
- Coustasse, A., Kimble, C., and Maxik, K. (2020). Rethinking Supply Chain Management Strategies for Ventilator Related Medications during COVID-19 Pandemic in the United States. Int. J. Health. Management 13, 352–354. doi:10.1080/20479700.2020.1801162
- Demissie, H., & Hanlin, R. (2015). Local Supply Chains for Medicines and Medical Supplies in Kenya: Understanding the Challenges. Nairobi: African Centre for Technology Studies.
- Dill, S., and Ahn, J. (2014). Drug Shortages in Developed Countries-Reasons, Therapeutic Consequences, and Handling. Eur. J. Clin. Pharmacol. 70, 1405–1412. doi:10.1007/s00228-014-1747-1
- Fatima, S. A., and Khaliq, A. (2017). A Survey Regarding Drug Shortage in Tertiary Care Hospitals of Karachi, Pakistan. Jppcm 3, 262–266. doi:10.5530/jppcm.2017.4.69
- Farinde, A. (2017). Drug Action. Columbia Southern University.
- Gebremariam, E.T., Gebregeorgise, D.T. and Fenta, T.G. (2019) ‘Factors contributing to medicines wastage in public health facilities of South West Shoa Zone, Oromia Regional State, Ethiopia: A qualitative study’, Journal of Pharmaceutical Policy and Practice, 12(1). Available at: https://doi.org/10.1186/s40545-019-0192-z.
- Hakuzimana, T. et al. (2021) ‘Assessment of Factors Contributing to Medicine Expiry in Rwanda: Case of the Medical Procurement and Production Division’, Rwanda Journal of Medicine and Health Sciences, 4(2), pp. 281–291. Available at: https://doi.org/10.4314/rjmhs.v4i2.7.
- General, A. (2015). Report of the Auditor General on the accounts of the Republic. Lusaka: Office of the Auditor General.
- General, A. (2016). Report of the auditor general on the accounts of the Republic. Lusaka: Office of the Auditor General.
- Gerba, H. (2018). Strengthening the pharmaceutical supply chain to deliver quality medicines in Ethiopia and across Africa. Addis Ababa.
- Govindaraj, R., Reich, M., & Cohen, J. (2000). World Bank Pharmaceutical, Human Development Network (HNP) Discussion Paper, the World Bank. Washington D.C.
- Iqbal, M., Geer, M., & Dar, P. (2017). Medicines Management in Hospitals: A Supply Chain Perspective. Systematic Reviews in Pharmacy, Vol 8, Issue 1, 80-85.
- Jahanbani, E., Shakoori, R., & Kahkesh, M. (2016). Drug Supply Chain Management and Implementation of Health Reform Plan in Teaching Hospital Pharmacies of Ahvaz, Iran. Hospital Practices and Research.
- Kwan, A. (2014). Inventory of Information and Communication Technology Solutions for Supply Chains.
- Kapoor, D. (2018) ‘An Overview on Pharmaceutical Supply Chain: A Next Step towards Good Manufacturing Practice’, Drug Designing & Intellectual Properties International Journal, 1(2), pp. 49–54. Available at: https://doi.org/10.32474/ddipij.2018.01.000107.
- Mashishi, K. A. (2015). Expiration of drugs in public hospital pharmacies of Sekhukhune district, Limpopo province, South Africa. Limpopo.
- NAHAMY, D. (2007). Assessment of essential drug management in the public health facilities in Uganda.
- Sharma, S., & Chaudhury, R. (2015). Improving Availability and Accessibility of Medicines: A Tool for Increasing Healthcare Coverage. ARCHIVES OF MEDICINE Vol. 7 No. 5:12, 1-9.
- Health Systems & ReformVolume 5, 2019 – Issue 2. Improving Supply Chain for Essential Drugs in Low-Income Countries: Results from a Large-Scale Randomized Experiment in Zambia.
- Awol Jemal et al., 2019. Unused and Expired Medications: Are They a Threat? A FacilityBased Journal of Primary Care & Community Health, 11© The Author(s) 2019 Article reuse guidelines:sagepub.com/journals-permissions.
- Basaza, R., Alier, P. K., Kirabira, P., Ogubi, D., & Lako, R. L. L. (2017). Willingness to pay for National Health Insurance Fund among public servants in Juba City, South Sudan: A contingent evaluation. International Journal for Equity in Health, 16(1), 158. https://doi.org/10.1186/s12939-017-0650-7
- Bashaar, M., Thawani, V., Hassali, M. A., & Saleem, F. (2017). Disposal practices of unused and expired pharmaceuticals among the general public in Kabul. BMC Public Health, 17(1), 45. https://doi.org/10.1186/s12889-016-3975-z
- Building Pharmaceutical Management Capacity in South Sudan. (2017). (January).
- Bukhari, S. K. S., Qureshi, J. a R. H., Jooma, R., Bile, K. M., Kazi, G. N., Zaibi, W. a, & Zafar, A. (2010). Essential medicines management during emergencies in Pakistan. Eastern Mediterranean Health Journal, 16, 106–113.
- Celeste Sauls. 2016. Trend in revenue loss due to expired medication at a large urban hospital in Johannesburg, South Africa A Research Report Submitted to the School of Public Health, University of the Witwatersrand in Partial Fulfilment of the Requirements for the Degree of Master of Public Health Student number: 445783
- Ebaidalla, E. M., & Ali, M. E. M. (2017). Determinants and Impact of Households’s Outof-Pocket Health Care Expenditure in Sudan: Evidence From Urban and Rural Population. Presented at the Economic Research Forum Working Papers.
- Embrey, M. (2011). Toward Sustainable Access to Medicines. Management Sciences for Health. Retrieved from https://apps.who.int/medicinedocs/documents/s19577en/s19577en.pdf
- Hertog, M. L. A. T. M., Uysal, I., McCarthy, U., Verlinden, B. M., & Nicolaï, B. M. (2014). Shelf life modelling for first-expired-first-out warehouse management. Philosophical Transactions. Series A, Mathematical, Physical, and Engineering Sciences, 372(2017). https://doi.org/10.1098/rsta.2013.0306
- Iqbal, M. J., Geer, M. I., & Dar, P. A. (2017). Medicines Management in Hospitals : A Supply Chain Perspective. 8(1), 80–85.
- Kamba, P. F., Ireeta, M. E., Balikuna, S., & Kaggwa, B. (2017). Threats posed by stockpiles of expired pharmaceuticals in low- and middle-income countries: A Ugandan perspective. Bulletin of the World Health Organization, 95(8), 594–598. https://doi.org/10.2471/BLT.16.186650
- Nakyanzi et al., (2009) Bulletin of the World Health OrganizationPast issuesVolume 88: 2010Volume 88, Number 2, February 2010, 81–
- Mani, A., & Thawani, V. (2019). The persisting environmental problem of disposal of expired and unused medicines. Journal of Mahatma Gandhi Institute of Medical Sciences, 24(1), 13.
- Manyazewal, T. (2017). Using the World Health Organization health system building blocks through survey of healthcare professionals to determine the performance of public healthcare facilities. Archives of Public Health, 75. https://doi.org/10.1186/s13690-017-0221-9
- Mashishi, K. A. (2015). Expiration of drugs in public hospital pharmacies of Sekhukhune District, Limpopo Province, South Africa.
- Mathew, J., & John, J. (2013). New Trends in Healthcare Supply chain.
- Mhlongo, N. F. (2014). Transparency in supply chain management: a South African local government case analysis.
- MoH, 1993. National drug policy and authority statute. Kampala: Republic of Uganda; 1993.
- MoH, 2006. Value for money audit report on the management of health programmes in the health sector. Kampala: Ministry of Health; 2006.
- MoH, 2011. Guidelines on Safe use of High Alert Medications, Pharmaceutical Services Division, Malaysia.
- National Assembly of Zambia (2022) ‘Follow – Up Audit Report on the Performance Audit on the’.
- Tull, K. (2018). Drug expiry standards in developing countries.
- Tumwine, Y., Kutyabami, P., Odoi, R. A., & Kalyango, N. (2010). Availability and Expiry of Essential Medicines and Supplies during the ‘Pull’ and ‘Push’ Drug Acquisition Systems in a Rural Ugandan Hospital. 9(March), 557–564.
- Vledder, M. et al. (2019) ‘Improving Supply Chain for Essential Drugs in Low-Income Countries: Results from a Large Scale Randomized Experiment in Zambia’, Health Systems and Reform, 5(2), pp. 158–177. Available at: https://doi.org/10.1080/23288604.2019.1596050
- WHO(2016). Guidelines for Redistribution of Excess and Near-expiry Essential Medicines Between Public Health Facilities in South Sudan. May 2016. Retrieved June 20, 2019, from http://apps.who.int/medicinedocs/en/m/abstract/Js23208en/
- WHO(2019). Global Health Expenditure Database [Database]. Retrieved July 2, 2019, from Data Explorer website: http://apps.who.int/nha/database/Select/Indicators/en
- World Health Organization. (2010). Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. World Health Organization.